Experts Matter. Find Yours.
Connect for media, speaking, professional opportunities & more.

New prostate cancer urine test shows how aggressive disease is and could reduce invasive biopsies
Researchers from the University of East Anglia have developed a new urine test for prostate cancer which also shows how aggressive the disease is. A new study shows how an experimental new test called ‘ExoGrail’ has the potential to revolutionise how patients with suspected prostate cancer are risk-assessed prior to an invasive biopsy. The research team say their new test could reduce the number of unnecessary prostate cancer biopsies by 35 per cent. Prostate cancer is the most common cancer in men in the UK. It usually develops slowly and the majority of cancers will not require treatment in a man’s lifetime. The most commonly used tests for prostate cancer include blood tests, a physical examination known as a digital rectal examination (DRE), an MRI scan or an invasive biopsy. However, doctors struggle to predict which tumours will become aggressive, making it hard to decide on treatment for many men. Lead researcher Dr Dan Brewer, from UEA’s Norwich Medical School, said: “While prostate cancer is responsible for a large proportion of all male cancer deaths, it is more commonly a disease men die with rather than from. “Therefore, there is a desperate need for improvements in diagnosing and predicting outcomes for prostate cancer patients to minimise over-diagnosis and overtreatment whilst appropriately treating men with aggressive disease, especially if this can be done without taking an invasive biopsy. “Invasive biopsies come at considerable economic, psychological and societal cost to patients and healthcare systems alike.” The research team developed the new ExoGrail urine test by combining two biomarker sources - measurements of a protein-marker called EN2 and the levels of gene expression of 10 genes related to prostate cancer risk. It builds on previously developed tests called PUR and ExoMeth. They tested it using urine samples from 207 patients who had been undergone a biopsy for prostate cancer at the Norfolk and Norwich University Hospital (NNUH). When the urine results were compared to biopsy results, the study showed that the test had successfully shown which patients had prostate cancer and which did not. The ExoGrail test also provided risk scores for patients and highlighted those for which an invasive biopsy would have been beneficial. The findings show that using information from multiple, non-invasive biomarker sources has the potential to greatly improve how patients with suspected prostate cancer are risk-assessed prior to an invasive biopsy. Dr Brewer said: “Our new urine test not only shows whether a patient has prostate cancer, but it importantly shows how aggressive the disease is. This allows patients and doctors to select the correct treatment. And it has the potential to reduce the number of unnecessary biopsies by 35 per cent.” The research team was led by Dr Shea Connell, Prof Colin Cooper, Dr Daniel Brewer and Dr Jeremy Clark, all from UEA’s Norwich Medical School, in collaboration with the Norfolk and Norwich University Hospital, the University of Surrey, the University of Bradford, The Earlham Institute, and The Movember GAP1 Urine Biomarker Consortium. The urine biomarker research was funded by the Movember GAP1 Urine Biomarker project, Prostate Cancer UK, The Masonic Charitable Foundation, The Bob Champion Cancer Trust, the King family, The Andy Ripley Memorial Fund, the Hargrave Foundation, Norfolk Freemasons and the Tesco Centenary Grant. Paul Villanti, executive director of programmes at Movember, said: “We are proud to have supported the development of the ExoGrail urine test as part of our Global Action Plan Urine Biomarker project. “Having non-invasive tests which can accurately show how aggressive a man’s prostate cancer is not only reduces the number of men having to undergo painful biopsies, but also ensures that the right course of treatment for the patient is selected more quickly.” ‘Integration of Urinary EN2 Protein & Cell-Free RNA Data in the Development of a Multivariable Risk Model for the Detection of Prostate Cancer Prior to Biopsy’ is published in the journal Cancers on Tuesday, April 27, 2021.


What Can A Forgotten Piece of Our Opioid Addiction and Treatment History Teach Us?
As the nation struggles with the third wave of a continuing opioid epidemic, a newly republished book co-authored by Nancy Campbell, the head of the Department of Science and Technology Studies at Rensselaer Polytechnic Institute, offers insight into present-day drug addiction and treatment by exploring a complex chapter from the nation’s past. Written with JP Olsen and Luke Walden, The Narcotic Farm: The Rise and Fall of America’s First Prison for Drug Addicts details the history of the United States Narcotic Farm, a federal institution that opened in 1935 outside of Lexington, Kentucky. Jointly operated from 1935 to 1975 by the U.S. Public Health Service and the Federal Bureau of Prisons, the Narcotic Farm was a combination prison, hospital, working farm, rehabilitation center, and research laboratory. “All of our scientific knowledge about human opioid addiction comes from that time, comes from that place,” said Campbell, a leading figure in the social history of drugs, drug policy, and harm reduction, on an episode of the Landmark Recovery Radio podcast. The facility, which was also the subject of a 2009 documentary featuring Campbell, has a complicated legacy. It revolutionized treatment methods commonly accepted today, such as using methadone to medically manage heroin detox and the development of drugs like naloxone and buprenorphine. But it fell under a cloud of suspicion in 1975, when Congress learned that researchers had recruited patients as test subjects for CIA-funded LSD experiments as part of the notorious MK-Ultra project. “With the ongoing opioid epidemic worsening this past year in the midst of the COVID-19 pandemic, the lessons learned in this book continue to be relevant today,” Campbell said. Campbell is also the author of Using Women: Gender, Drug Policy, and Social Justice and Discovering Addiction: The Science and Politics of Substance Abuse Research, as well as the co-author of Gendering Addiction: The Politics of Drug Treatment in a Neurochemical World. Her most recent book, OD: Naloxone and the Politics of Overdose, was published in 2020. “Nobody should die of overdose. A high overdose death rate signals that we have not cared for the people who have been hurt most by the war on drugs, first pursued by President Dwight D. Eisenhower in 1954,” Campbell said in a recent “Academic Minute” segment. Campbell is available to discuss a wide range of topics relating to drug policy and history, including the Narcotic Farm.



Is hospital advertising actually good for our health?
Hospitals and healthcare organizations in the U.S. spend $1.5 billion on advertising every year. It’s a topic that provokes lively debate and a certain amount of controversy. Medical bodies, policy makers, and scholars alike question the ethics and efficacy of using (constrained) budgets to promote hospitals to patients. Diwas KC, professor of information systems & operations management at Emory University’s Goizueta Business School, and Tongil Kim, an assistant professor of management at Naveen Jindal School of Management in Texas, conducted a large-scale study of hospitals and patients in the state of Massachusetts to better understand the impact of hospital advertising. What they found is striking: Not only does television advertising work, it significantly drives demand, attracting patients living far from the hospital and beyond its regular area. And that’s not all. KC and Kim discovered that limiting hospital advertising or imposing an outright ban, as some groups have called for, might actually have serious negative effects on patient healthcare. “There has been a lot of discussion about banning advertising over recent years because of uncertainties around wasting money and resources,” KC said. In the paper “Impact of hospital advertising on patient demand and outcomes,” KC shows that there is a correlation between the amount spent on TV advertising and the quality of the hospital in question. Healthcare facilities that invest more in advertising tend to be “better” hospitals, he adds; they offer higher caliber care and services and, as such, they see much lower patient readmission rates—a key quality metric in healthcare. To get to these insights, KC and Kim looked at more than 220,000 individual patient visits to hospitals in the state of Massachusetts over a 24-month period. Among the data they collected were things like hospital type, location, and dollars spent on advertising. Patients were documented in terms of medical conditions, insurance, zip codes (to determine residence), and median household income. They were able to contrast those hospitals that invested in television advertising and those that did not. With the former, they uncovered a significant uptick in patient visits, with people coming from far further afield. This was particularly true of wealthier patients. Then there’s the question of patient outcomes. Here the data showed unequivocally that it’s the high-quality, low-readmission hospitals that advertise more—something that KC attributes to the natural tendency to get “more bang for the advertising buck when the quality of your product or service is better.” As for banning advertising, this would negatively impact these hospitals, he argues, limiting their ability to attract patients. It could also lead to an increase in population-level readmission rates. “Patient readmission rates are one of the key metrics along with mortality rates that tell us how well a healthcare facility is working,” said KC. “If a patient gets discharged but has to come back to a hospital in, say, 30 days, unless it’s a chronic condition or ongoing treatment, it’s a good indication that the patient didn’t get the level of care they should have the first time.” Indeed, “when we looked at all of the data, we found that the hospitals where there were fewest revisit rates were those that advertised more,” he said. KC finds that a blanket ban on hospital advertising could lead to an extra 1.2 readmissions for every 100 patients discharged. It’s a significant and “surprising” finding. And one that should inform the debate around healthcare advertising spend in the U.S. “There’s also the idea that this is a zero-sum game because if a patient doesn’t go to hospital A, they’re just going to go to hospital B—the one that advertises more—splitting the pie in different ways but not increasing that pie,” KC said. “What our study finds is that yes, advertising does draw patients away from one facility and towards another, but that the latter generally delivers better patient outcomes,” he said. “So, there is a social welfare benefit right there that suggests that you should not ban hospital advertising. There are real health benefits in allowing [advertising] to happen.” If you are a journalist looking to cover this topic - then let our experts help. Diwas KC is a Professor of Information Systems & Operations Management at Emory University’s Goizueta Business School. He is an expert in the areas of Data Analytics, Operations, and Healthcare. If you are interesting in arranging an interview - simply click on his icon to set up a time today.



The initial doses of the first approved COVID-19 vaccine are here, and health care workers are part of the group that’s getting it first. One of them is Dr. David Banach, UConn Health infectious diseases physician and hospital epidemiologist, who sees the vaccine not only as a major breakthrough in the fight to end the pandemic, but also as an opportunity for his clinical colleagues to lead that effort and set the tone for the rest of the world. Here are some key facts about the COVID-19 vaccine, with Dr. Banach providing explanations of each: The COVID-19 vaccine won’t infect you with COVID-19. “There is no live virus in this vaccine, so you can’t actually get infected with SARS-CoV-2 from the vaccine. What this vaccine has is messenger RNA, which is a little bit of genetic code that allows the body’s natural machinery to make the protein that will generate an immune response." You may actually want some side effects from the COVID-19 vaccine. “You might get some soreness at the injection site, maybe some fatigue for a day or two, but that can be a good thing, a sign your body is making that immune response. That’s what is going to protect you in the future if you get exposed to the virus. The data from the clinical trials show the side effects – the soreness, fatigue, in some cases a short-lived fever – occur the first few days afterwards, and the rate of serious side effects is extraordinarily low for this vaccine.” The vaccine was developed relatively quickly, but not by compromising the scientific process. “When you look at Operation Warp Speed and how this process moved really quickly, that was really focused on the research and development piece and the manufacturing piece. Importantly, the phase 3 clinical trial was not rushed. This is the same type of clinical trial that we would do for any other vaccine. We followed people for at least two months. The clinical trials were huge, and they had diverse populations. So that part of the whole process wasn’t rushed at all, and that’s the most important part.” Don’t throw out those masks just yet. “We know this vaccine prevents people from developing symptomatic and severe COVID infection. I think what we don’t know is the effect it’s going to have on viral transmission, including asymptomatic shedding of virus. For instance, people who get the vaccine might still potentially shed virus, potentially at a lower level. The vaccine will prevent them from actually becoming ill, but vaccinated individuals might still be able to have virus in their nose and their respiratory system. Immunity from the vaccine is not instantaneous. “The COVID-19 vaccine clinical trials using the Pfizer-BioNTech and Moderna mRNA vaccines were designed using a two-dose series in order to generate the optimal level of protection from the vaccine. That’s why getting both doses of the vaccine is essential. Although there is likely some individual variability, immunity may not be optimal until several days after the second dose. The phase 3 clinical trials used a period of at least one-to-two weeks after the second dose as a marker of immunity during which they were able to demonstrate the efficacy of the vaccines in protecting against COVID-19 infection.” Dr. David Banach is one of the lead experts on COVID-19 in America. He is available to speak with media regarding the vaccination and what the future holds with regards to COVID-19. To book an interview – simply click on his icon and arrange a time now.


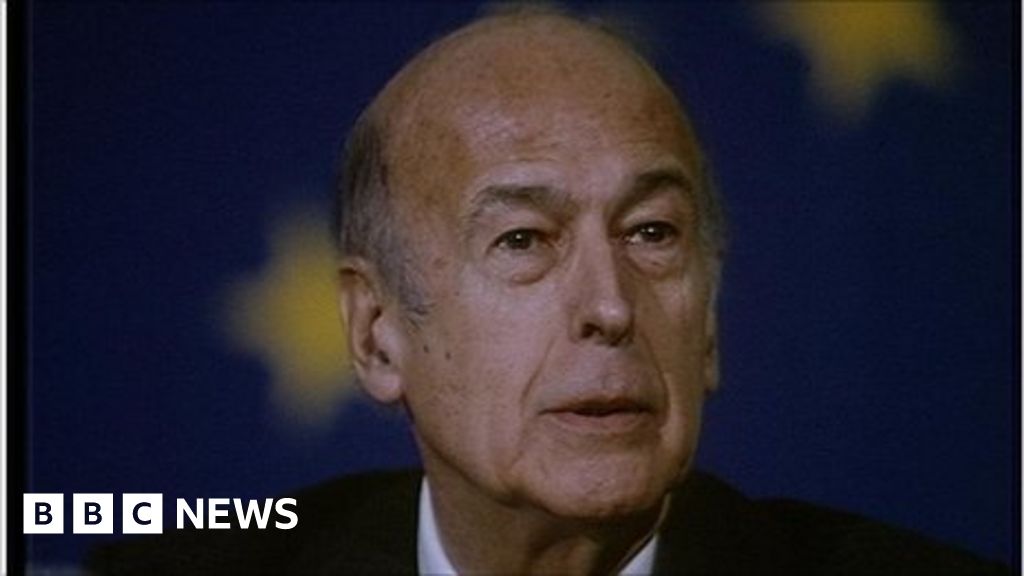
Dr David Lees from the School of Modern Languages and Cultures at the University of Warwick said: “France has lost a fascinating political leader. “Valery Giscard d’Estaing, who has died aged 94, was a modernising if controversial President of the Fifth French Republic between 1974 and 1981. “Giscard was the first non- Gaullist president of the Republic and signalled an end to the continuity following de Gaulle’s presidency. Giscard was an ardent Europhile and one of the architects of the European Constitution that was rejected by the French in 2005. In the course of his presidency, Giscard was responsible for pushing through the reduction in the age of voting to 18, the Veil reforms which legalised abortion and major changes to cultural policy. Giscard was very active in foreign policy, becoming embroiled in a scandal over diamonds gifted to him by the dictator Jean-Bedel Bokassa of the Central African Republic. “The legacy of Giscard remains one of modernity mixed with controversy. Having recently been accused of sexual misconduct, Giscard continued this trend until his death in hospital in Tours in this most exceptional of years.”


Criminals are opportunists, and the COVID-19 global onslaught has brought with it not just health threats but cybersecurity risks, too. Within weeks of the COVID-19 outbreak, hackers have already commandeered the virus to unleash cyberattacks, sending emails purporting to provide coronavirus guidance laced with cyberattack software. In one more alarming case, they appear to have attacked a hospital and forced it to cancel operations and take key systems offline. As the outbreak continues to intensify, the UK National Cyber Security Centre (NCSC) warned that the volume of these attacks will likely increase, pointing to the increased registration of coronavirus-related webpages. Criminals are opportunists, and the COVID-19 global onslaught has brought with it not just health threats but cybersecurity risks, too. As companies move to protect the health of their workforce, it’s also important to protect the systems they’re using to run their businesses. It’s especially important for hospitals to shore-up their cyber defenses. If they don’t, just as they are racing to respond to COVID-19, they could face situations like University Hospital Brno in the Czech Republic, which earlier this month was forced to divert patients and cancel planned operations while it worked to address an attack. The most likely cyber threats are email “phishing” campaigns that use the coronavirus as a lure to get the recipient to open an attachment that contains malware. According to the NCSC, such “phishing” attempts are happening on a global scale in multiple countries, which has led to both a theft of money and sensitive data. Similarly, known hacker groups have been launching websites purporting to sell masks or other safety-related measures for coronavirus, possibly to use them as another vector for cyberattacks. The NCSC has also cautioned that these attacks are “versatile and can be conducted through various media, adapted to different sectors and monetized via multiple means, including ransomware, credential theft, bitcoin or fraud.” The cybersecurity firm ProofPoint has seen a rise in these cyberattack emails with COVID-19 themes since January. Both ProofPoint and IBM’s X-Force cybersecurity unit identified a campaign that targeted users in Japan with an email masquerading as a coronavirus information email that carries with it a potent type of cybercrime software. In the US, the Secret Service recently warned of scams from online criminals posing as sellers of high-demand medical supplies to prevent coronavirus. They’ll require payment upfront and not send the products. Cyber criminals have also been posing as the World Health Organization and the US Centers for Disease Control and Prevention (CDC), sending fraudulent emails from the former and “creating domain names similar to the CDC’s web address to request passwords and even bitcoin donations to fund a vaccine” for the latter. In addition to the use of the coronavirus as a cyberattack vector, the growing need for working remotely to mitigate the spread of COVID-19 has increased companies’ exposure to cyber threats. The increase in remote work creates more opportunities for hackers to make inroads from less secure locations. Companies should also ensure they can provide adequate security when their whole workforce is remote. They should quickly work through the security implications of workers choosing to switch to insecure personal devices. With national-level pressures on home broadband, staff will also resort to mobile hotspots, which are often less secure. And enabling remote connectivity at scale, with the right security configurations, can be a challenge even with months of preparation time. A recent US Department of Homeland Security COVID-19 cybersecurity notice pointed to the importance of making sure that security measures are up to date for companies’ remote access systems. Additional measures to consider include enabling multifactor authentication—which can require two or more steps to verify a user’s identity before granting access to corporate networks. The NCSC is also working to identify malicious sites responsible for phishing and cyberattack software. A final looming cyberthreat related to Covid-19 is disinformation. The World Health Organization and other agencies have for months been combatting disinformation campaigns spreading false information about the origins of and treatments for COVID-19—reports that seed more confusion and increase risks to society. All of that means that computer virus risks are emerging as the biological virus spreads—and both are a threat to business. Cyber risk mitigation efforts should account for the different ways that a company can be affected, including impacts on the technical, operational, legal and reputational aspects of a business. Often, the reputational effects of a cyberattack are more significant than direct the business or technical impact. To mitigate all of the potential impacts of cyberattacks taking advantage of the Covid-19 outbreak, companies should: Review and update crisis and cybersecurity response plans, and ensure internal and external communications response plans are robust. Confirm that members of the crisis management team understand their roles and responsibilities. Make sure all communications channels have the latest security patches. Review and update access controls, particularly when remote access is used heavily, to make sure that only those who require access to sensitive systems to do their jobs have it. Take extra care when handling medical information. For companies managing employees who have contracted Covid-19, it’s important that personal health information is handled with strong security measures, including encryption. Educate employees about the cyber risks that may attempt to capitalize on fear of the Covid-19 virus—whether it be phishing email or disinformation. Covid-19 poses a number of short- and long-term challenges to business resilience, and the virus’s trajectory is quick and unpredictable. But it’s possible to anticipate and mitigate a number of the cyber threats that will try to ride the virus’s coattails. The companies that do will be more resilient and better positioned to withstand the direct health and operational effects of the virus.



When the first cases of the novel coronavirus arrived in Chatham County, Georgia, Rafael Agosto, who has been a respiratory therapist at St. Joseph’s/Candler Hospital in Savannah for 17 years, had to recalibrate his approach to lung care. “Initially, it was kind of wild because we didn’t know what to expect and how to manage any of these patients,” said Agosto. “What are we looking for, and how do we treat this?” The primary role of a respiratory therapist is to assist patients who have trouble breathing by administering oxygen, managing ventilators and measuring lung function, among other methods. COVID-19 symptoms include fatigue, fever, cough and shortness of breath, and at the onset, Agosto and his colleagues raced to stabilize patients who tested positive for the precarious disease. “We were trying to keep them oxygenated,” he said. “It was sort of like pneumonia, but we wouldn’t treat it like a normal pneumonia because it’s like a deadly pneumonia. Patients were declining very fast so you didn’t have time like you normally would with other patients. And they were of all ages. That’s what was so scary.” While grappling with patient care, Agosto and his co-workers were also dealing with fear for their own safety with exposure to the virus in such close proximity. St. Joseph’s/Candler, Agosto’s employer since he graduated with a B.S. in respiratory care from Georgia Southern University’s Armstrong Campus in 2003, made it a priority to outfit the health care workers with proper personal protection equipment (PPE), Agosto said. “That was scary but they made sure we had what we needed,” he explained. “Safety was the number one key. So the proper PPE, it was everything. We had all of it. A face shield, goggles, scrub cap and masks. They were not comfortable at all. At least here when I wore them I had downtime, but in Boston, holy moly, my face was bruised.” Agosto registered for a four-week rotation with a crisis nurse staffing company that placed him at Good Samaritan Medical Center in Brockton, Massachusetts, a suburb of Boston. COVID-19-related deaths in Massachusetts were outpaced only by New York and California, and Brockton was the second hardest-hit community in the state. “The reason I went was the opportunity to help patients, number one, and to learn how they were managing their ventilator patients there so it could help here,” he explained. On April 19, Agosto reported to the facility, suited up for his first 12-hour shift. “I was in complete shock when I got in there,” Agosto said. “The ICU was full. Every single floor was possible for COVID.” The hospital averaged 80 to 90 cases throughout his stay, and the intensive care unit remained full. Days were hectic and taxing; lunch was an afterthought. His focus was on keeping patients off of ventilators, as global reports show that more than half of ventilated coronavirus patients don’t survive. Yet, “it started becoming hard to get them off ventilators,” and his group often didn’t have a choice but to put patients on 100% oxygen. Stress didn’t let up, but Agosto found moments of solace in interactions with patients. “I would walk into patients’ rooms and they all kept telling me the same thing — they’re scared,” he said. “Because they don’t know anything. It’s like a ghost town because the nurses are running around. Patients felt they weren’t being seen much.” In response, Agosto offered his undivided attention. “That’s one thing that made me feel really good,” Agosto continued. “Just to sit there and talk with them for a few minutes. Or just listening to them. That’s what we’re here for, and they were appreciative.” Agosto returned to Savannah healthy and with a new oxygen delivery device to share with his co-workers at St. Joseph’s/Candler. His manager ordered the devices to serve local patients. “The most important thing I took out of this is that it’s serious, and people are doing everything they can,” Agosto said. “They’re putting their lives in jeopardy for the patients, and I’m glad I had the opportunity to do that.” The accomplishment of his goals in a time of crisis and his continued dedication as a respiratory therapist leave Agosto fulfilled. “I didn’t get sick,” he said. “I helped as much as I possibly could. I did what I wanted to achieve. I’m so happy and blessed because I still love my job.” If you’re a journalist covering COVID-19 and how Georgia Southern University is helping mitigate the spread of this virus – then let us help. Barry Joyner, Ph.D., is the dean of Georgia Southern University’s Waters College of Health Professions - simply click on his icon to arrange an interview today.



As the COVID-19 pandemic unfolded and healthcare organizations began experiencing shortages of personal protective equipment (PPE), faculty, staff and students at Georgia Southern University stepped up to fulfill a need. Making use of the 3D printers on the Statesboro and Armstrong campuses, as well as at the FabLab at the Business Innovation Group’s (BIG) downtown Statesboro location, the campus communities quickly began production of protective face shields and respirators. “We can’t afford to sit back and wait for things to happen,” said Dominique Halaby, DPA, director of the BIG. “We have to make them happen. We have this responsibility to make a difference, to be a part of that front line, whether it’s immediately in our community, our state or our respective area.” To date, the Department of Manufacturing Engineering has sent 200 3D-printed protective face shields with headbands to Augusta, Georgia, for healthcare workers at Augusta Medical Center, while the BIG has sent 100 face shields and 10 “Montana Masks,” a 3D-printable respirator filtration mask that can be fitted to a healthcare provider’s face and sanitized between uses, to Atlanta-area hospitals. The Department of Mechanical Engineering on the Armstrong Campus has also printed Montana Masks that will be delivered to workers in the St. Joseph’s/Candler Hospital System (SJCHS) in Savannah, Georgia, while the Respiratory Therapy Program in the Waters College of Health Professions donated 10 ventilators to the Georgia Emergency Management Agency. “I am unbelievably proud of our faculty, staff and students who have their own families to take care of, but are putting themselves on the line to help our medical professionals in this time of critical need,” said Mohammad Davoud, Ph.D., dean of the Allen E. Paulson College of Engineering and Computing. Wayne Johnson, Ph.D., professor of mechanical engineering, believes providing these materials to the Savannah community during a time of critical need is reinforcing a longtime commitment to the region. “The Armstrong Campus of Georgia Southern has a long history of working within the Savannah community, and during this pandemic, it was especially important for mechanical engineering faculty and students at the Armstrong Campus to step up during a time of great need,” said Johnson. “ Our work with SJCHS to develop, test and donate 3D-printed respirators may also lead to other research and development collaborations in the post-COVID-19 future.” In addition to benefiting area healthcare workers, Johnson believes this project is a great way for students to put their classroom skills into practice. If you would like to learn more about how the students, staff and faculty at Georgia Southern University are helping out during the COVID-19 crisis – the let our experts help. Wayne Johnson is an expert in additive manufacturing, mechatronics, biomechanics and engineering education. He is available to speak with media about this great initiative, simply click on his icon to arrange an interview today.
Diary of a COVID-19 crisis nurse in NYC: A Georgia Southern student’s first job
On May 1, Tucker Westbrook could finally sleep in. He’d been on duty as a COVID-19 crisis nurse at Harlem Hospital Center in New York City for 11 consecutive days, with a routine that began before the sun came up and ended long after the city had gone dark. Most mornings, he’d wake at 5:45 am., center himself with prayer and meditation, eat breakfast, and hop on a bus in time to clock in for his shift at the largest public hospital in Central Harlem by 7 a.m. Each day as he entered the halls of the facility’s surgical floor, which was transformed into a COVID-19 holding unit for the larger part of his three-week work rotation, he was unsure of what he’d encounter. Just weeks earlier, Westbrook, a May 2019 Georgia Southern University nursing graduate from Butler, Georgia, accepted a short-term contract to assist with the Coronavirus pandemic in the epicenter of the U.S. outbreak. This was Westbrook’s first professional job, following what was supposed to be a yearlong mission trip in Southeast Asia, but was cut short due to the pandemic, and nothing could fully prepare him for the impact of his initial experience. “The first day, I thought, ‘I’m not prepared for this,’” he admitted. “Those first few days I was on pins and needles and thought, ‘how am I going to mess up?’” The stakes were high. By the time he arrived in New York City, thousands had already been hospitalized, and many had died. Seasoned nurses and doctors were depleted and morale was low across the city, he explained on the phone as he looked out over a desolate Times Square from his hotel window. “They asked me, ‘why did you come here?’” Westbrook recalled. “And I said that I wanted to be, hopefully, a light in this dark place right now. The patients, the doctors, the nurses, the nursing assistants, the janitorial assistants — my goal is to learn everyone’s names and greet them with a smile behind my mask.” A friend encouraged Westbrook to look for a temporary nursing job upon his return from abroad. When he applied for highly competitive positions with a crisis staffing agency, he requested placement in an area hard hit by the pandemic. “Just like Southeast Asia, I wanted to go where there was the biggest need, and I had enough gifts to meet that need,” Westbrook said. This was Westbrook’s first trip to New York, and he stepped into a scene where images of makeshift morgues and ventilator shortages splashed across the media came to life in front of him. “It has been surreal to see,” he said. Assigned to provide cluster care to potential COVID-19-positive patients for minimal exposure, Westbrook also focused on simple acts of kindness to help ease increased anxiety among the patients. “That might be things as small as giving a wet rag to wipe their face,” Westbrook said. “It may be filling their jars with ice cold water in the morning. Whatever might help them feel more comfortable.” Westbrook’s patients were diverse: a teenage gunshot victim who sobbed at the prospect of being infected with the virus; an adult male who discussed intimate thoughts about death with his family over the phone; and a woman who was depressed until Westbrook sat with her so she didn’t feel alone. Experiencing humanity in its most delicate form was life-defining. “I was learning more about nursing care but also continuing to serve (my patients) beyond simply giving them medicine,” Westbrook said. “I was able to advocate for them with the doctor, especially without their families there. I’m learning how to go above and beyond, and what our job responsibilities are. I want to keep growing and learning to continue to give care to my patients.” The hospital staff also offered enormous support and guidance to Westbrook, who almost two weeks into the job felt exponentially more confident in his abilities. “If you had told me about any of this I wouldn’t believe it,” he said. “It has been incredible. I did not think I could do that at all, and here I am on the other side. This was such a lofty and high goal to complete this and do well. I’m thankful to even be here and have this opportunity.” Westbrook credits his father for encouraging him to study nursing, and Georgia Southern faculty for their expert instruction, which he put to use in New York, as well as their sage advice. “I wasn’t sure I was going to get my license,” he said. “My desire to become a doctor or a missionary became more and more compelling, but my professors assured me that it would be worthwhile to pursue my license, and they were right.” Following a quarantine in his family’s home, Westbrook will begin pre-medicine classes at Georgia Southern this summer. If you are a journalist looking to know more about Tucker’s story or the nursing program at Georgia Southern University – let us help with your coverage. Barry Joyner is the dean of Georgia Southern University’s Waters College of Health Professions - simply click on his icon to arrange an interview today.

Step aside Walking Dead – There’s another leading TV show being shot in Georgia now
When location scouts for NBC’s new television series “Council of Dads” combed Savannah for a realistic venue to shoot multiple hospital scenes, they knew they had found something special in the Health Professions Academic Building on Georgia Southern University’s Armstrong Campus. “I set up a visit, came and looked at it and I was floored,” said “Council of Dads” location scout and Armstrong Campus alumnus Anthony Paderewski. “I couldn’t believe it. Basically, you have a backlot for a TV show here. It was absolutely perfect for what we were looking for. So that being said, I went and I talked to the producers and I got some pictures. When I showed the pictures everyone was blown away.” “Council of Dads,” which premiered March 24 and now airs on Thursdays, is based on the book by Savannah native Bruce Feiler, and developed by former “Grey’s Anatomy” showrunners Tony Phelan and Joan Rater, who also serve as executive producers on the series. The story follows Scott Perry, a father of five who, after receiving a cancer diagnosis, asks a group of friends to step in as father figures to his children in the event that he isn’t around to see them grow up. “It’s an emotional family drama,” explained “Council of Dads” co-executive producer and producing director Jonathan Brown. “The idea is to try and be as real as possible. And the show is telling the story of a family and what it means to be a family in this day and age. It’s not just blood. The definition of family is growing, broadening with the types of relationships that are now included in a family. This is the story of one of those families that is made up of blood relationships, friendships, adoption and all those different kinds of things.” The show filmed almost entirely on location in the Savannah area for five months. Several of the scenes take place in a hospital, and the set has to be believable, multifaceted and offer the right aesthetic for television. Primarily, the true-to-life setting allows the University to provide exceptional education and training opportunities to help students succeed while addressing the healthcare needs of the region. The Waters College of Health Professions, housed in the Academic Building and Ashmore Hall, is the largest undergraduate health sciences college in the state of Georgia, and the University’s allied healthcare programs represent almost one-fifth of all undergraduate healthcare degrees earned in Georgia. “The use of the Health Professions Academic Building is validation that we are training our students for real-world health care settings,” said Barry Joyner Ph.D., dean of the Waters College of Health Professions. “The goal for the building was to simulate a hospital setting, and we have accomplished that.” Are you a journalist looking to cover this topic or learn how Georgia and Universities like Georgia Southern are working with film and television industries – the let us help with your stories. Barry Joyner is the dean of the Waters College of Health Professions at Georgia Southern University and is available to talk about this latest project on campus – simply click on his icon to arrange an interview today.