Experts Matter. Find Yours.
Connect for media, speaking, professional opportunities & more.

Election Watch 2025: Farnsworth Breaks Down Virginia’s Political Landscape
With early voting setting new records and national politics reshaping local elections, Professor Stephen Farnsworth is helping journalists and voters make sense of the noise. As director of the Center for Leadership and Media Studies at the University of Mary Washington, Farnsworth continues to be a go-to expert across major outlets. In just the past few weeks, he’s been featured in: • NBC Washington • WAMU • Yahoo News • Richmond Times-Dispatch • DC News Now • Virginia Mercury Farnsworth has weighed in on everything from Kamala Harris’ rising prospects to the effects of Trump’s policies on rural Virginia. Whether he’s speaking to the League of Women Voters or breaking down the numbers for DC news outlets, Farnsworth brings clarity to the chaos. For journalists covering Virginia politics and U.S. elections, Farnsworth is a key source of insight. Click on the icon below to connect with: Stephen Farnsworth, Professor of Political Science and International Affairs; Director, Center for Leadership and Media Studies Expertise: Virginia politics, media and messaging, U.S. elections, disinformation.


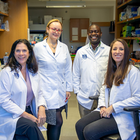
AU research team awarded $4.4 million American Heart Association grant
A research team at Augusta University, led by Jennifer C. Sullivan, PhD, has secured a $4.4 million grant from the American Heart Association to study the risk factors for cardiovascular and kidney diseases and how they impact women. Sullivan’s research center, “Disruptions in cardiorenal free fatty acid metabolism in Cardiovascular Kidney Metabolic Syndrome,” is part of a larger $15 million project titled “Strategically Focused Research Network on Cardiovascular Kidney Metabolic Syndrome: Heterogeneity in Women.” The overarching AHA project is aimed at learning why women may be more likely to develop cardiovascular and kidney diseases due to certain unique risk factors and life stages. Research teams from Massachusetts General Hospital and The Ohio State University were also chosen. “I think this is a huge step for Augusta University as we continue to distinguish ourselves and the research that we have here focused on the health of women,” said Sullivan, dean of The Graduate School. “This grant is particularly impactful as we look to advance and improve the health of women, not just in Georgia, but for the entire country.” According to the Healthy Georgia Report, produced by AU’s School of Public Health, Georgia has the 23rd highest rate of obesity in the United States. Among the women living in the state, 38.3% of them, as well as 37.5% of people living in rural areas, suffer from obesity. “It’s great that we are able to represent the state of Georgia because our state has such a high prevalence for obesity rates,” said Sullivan, who is the director of AU’s SCORE project “Improving awareness of women with hypertension: ROAR (Rural, Obese, At Risk).” “It’s important for us to understand that different populations have distinct needs. You can’t talk about a one-size-fits-all approach to health. This is really about trying to understand how different groups are impacted.” Each center is comprised of three teams, as well as a training component and an area partner. Together, they will explore obesity’s lifetime impact on CKM syndrome through three projects. CKM syndrome is a clinical term that describes the combined health effects of heart disease, kidney disease, diabetes and obesity, which puts people at high risk for heart attack, stroke and heart failure. According to the American Heart Association’s 2025 Heart Disease and Stroke Statistics, about 1 in 3 U.S. adults has at least three components of CKM syndrome, which include high blood pressure, abnormal cholesterol, high blood glucose (sugar), impaired kidney function and excess body weight. The first project is led by Daria Ilatovskaya, PhD, and Justine Abais-Battad, PhD, and will look at aging and Western diet-induced CKMS mechanisms in obesity. Ilatovskaya is an associate professor and the graduate program director for the Doctor of Philosophy in Physiology program, and Abais-Battad is an assistant professor in the Department of Physiology with the Medical College of Georgia at Augusta University. The second component, led by Jessica Faulkner, PhD, an assistant professor in MCG’s Physiology department, will study obesity-associated mechanisms of CKMS in pregnancy. The third project, led by Stephen Coughlin, PhD, with Marlo Vernon, PhD, is looking at CKMS epidemiology, associations with obesity, CVD/CKD. Coughlin is the program director for the Master of Science in Epidemiology and professor of epidemiology in the School of Public Health’s Department of Biostatistics, Data Science, and Epidemiology, while Vernon is an associate professor with MCG’s Georgia Prevention Institute and SPH’s Department of Community and Behavioral Health Sciences. Additionally, the team will talk to women and health care providers from a variety of backgrounds and experiences to assess current knowledge and interest levels in heart health and use that information to develop programs that may help treat and prevent disease. There is also a training director, Alison Kriegel, PhD, a professor in the Department of Physiology, and a core director, Guido Verbeck, PhD, chair and professor of the Department of Chemistry and Biochemistry in the College of Science and Mathematics. “We have a strong blend of clinical epidemiology and basic science, as well as a training component, which we will fill with post-doctoral fellows,” Sullivan said. “Dr. Ilatovskaya, Dr. Faulkner, Dr. Abais-Battad and Dr. Vernon are all a part of our ROAR grant, and, while this isn’t directly related to that program, it allowed us to demonstrate how we are already well positioned to work together to amplify our ability and increase awareness about the importance of the health of women.” The team has over 50 collaborative papers and has secured more than $13 million in collaborative funding to advance the health of women. They also all have experience training fellows and students to continue to expand their reach. “We already have a lot of the infrastructure in place for this kind of cross-disciplinary project, so we leaned very heavily into our connections and the expertise we have here at Augusta University. It’s set up very similar to our ROAR program, so this is something that was really organic in nature,” Sullivan said. The American Heart Association has invested almost $300 million to establish 18 Strategically Focused Research Networks, each aimed at addressing a key strategic issue identified by the association’s volunteer Board of Directors. Prior networks have been studying a wide variety of important topics including, but not limited to, prevention, hypertension, the health of women, heart failure, obesity, vascular disease, atrial fibrillation, arrhythmias/sudden cardiac death, cardiometabolic health/type 2 diabetes, health technology, cardio-oncology, the biological impact of chronic psychosocial stress and the role of inflammation in cardiovascular health. Each network centers around scientific knowledge and knowledge gaps, prevention, diagnosis and treatment of the key research topic. Three to six research centers make up each network, bringing together investigators with expertise in basic, clinical and population/behavioral health science to find new ways to diagnose, treat and prevent heart disease and stroke. Funding scientific research and discovery through initiatives like these awards is a cornerstone of the century-old American Heart Association’s lifesaving mission. The association has now funded more than $5.9 billion in cardiovascular, cerebrovascular and brain health research since 1949, making it the single largest non-government supporter of heart and brain health research in the United States. New knowledge resulting from this funding continues to save lives and directly impact millions of people in every corner of the U.S. and around the world. Looking to know more about the amazing research happening at Augusta? To connect with Dr. Sullivan, simply click on her icon to arrange an interview today.




10th Anniversary of the Supreme Court Legalizing Gay Marriage
The 10th anniversary of the U.S. Supreme Court’s landmark decision in Obergefell v. Hodges marks a decade since same-sex marriage became legal nationwide—a pivotal moment in the advancement of LGBTQ+ rights and civil liberties. This anniversary is newsworthy not only because of the social and legal progress it symbolizes but also due to ongoing conversations around equality, representation, and protection under the law. As the political landscape shifts and new challenges emerge, revisiting the legacy of this decision offers an opportunity to reflect on progress, examine setbacks, and spotlight the voices shaping the next chapter in LGBTQ+ advocacy. Key story angles that may interest a broad audience include: Personal stories from couples and families: Exploring how the decision transformed lives and created new definitions of family, love, and legal recognition. The legal legacy of Obergefell v. Hodges: Analyzing the impact on subsequent LGBTQ+ rights cases and how the precedent continues to be tested in courts. Backlash and resistance: Investigating the rise of anti-LGBTQ+ legislation and rhetoric in the decade following the ruling. Intersectionality within the LGBTQ+ rights movement: Highlighting the experiences of LGBTQ+ people of color, transgender individuals, and rural communities. The global ripple effect: Examining how the U.S. ruling influenced marriage equality movements in other countries. The future of LGBTQ+ rights: Discussing what comes next in the fight for inclusive healthcare, anti-discrimination laws, and gender identity recognition. Connect with our experts about the 10th Anniversary of the Supreme Court Legalizing Gay Marriage: Check out our experts here : www.expertfile.com

MEDIA RELEASE: Provincial Trunk Highway 34 Named the Worst Road in Manitoba
Manitobans have spoken – and the results are in. The 2025 CAA Worst Road is Provincial Trunk Highway 34 (PTH 34) in Central Plains/Pembina Valley, Manitoba. Frustrations with potholes, poor road maintenance, poor road signage and unpaved roads pushed PTH 34 to the number one spot. This marks this road’s sixth appearance on the CAA Worst Roads Top 10 list; however, this is the first time it has taken the top spot. This year also marks a historic first for the CAA Worst Roads campaign – for the first time in its 14-year history, nine out of ten roads on the top 10 list are from rural Manitoba communities. Saskatchewan Avenue, the only Winnipeg road on the list in 2025, has appeared on the CAA Worst Roads list for the last seven consecutive years. "The CAA Worst Roads campaign provides a powerful snapshot to governments on where to prioritize budgets and move up road repairs by giving Manitobans an opportunity to have their say on the difficulties they are experiencing in getting around," says Ewald Friesen, manager of government and community relations for CAA Manitoba, "We saw the proof of this when last year's winner, 18th Street in Brandon, received a swift and coordinated response from governments on the same day the results were released, with shovels in the ground by Fall.” This year’s campaign saw an almost 50 per cent increase in roads nominated, with 723 different roads across 86 municipalities. CAA research shows that 39 per cent of respondents expressed dissatisfaction with road work projects, stating that the roads don’t last long before they must be repaired again. However, 88 per cent are willing to put up with the inconvenience of construction in exchange for long-term improvements. "Manitobans take to this campaign because they are hopeful for change,” says Friesen. “CAA’s annual campaign plays a critical role in highlighting the roads that need urgent attention, providing governments with a better understanding of where Manitobans want these investments made." Half of the roads on the top 10 list are new this year. These include Provincial Road 234 in Interlake, Provincial Road 349 in Westman, Provincial Road 239 in Interlake, 26th Street in Brandon, and Provincial Trunk Highway 12 in Eastman. Manitoba's Top 10 Worst Roads for 2025 1. Provincial Trunk Highway 34, Central Plains/Pembina Valley 2. Provincial Road 234, Interlake 3. Provincial Road 307, Whiteshell 4. Provincial Road 239, Interlake 5. Provincial Road 349, Westman 6. 26th Street, Brandon 7. Provincial Trunk Highway 12, Eastman 8. Provincial Trunk Highway 26, Central Plains 9. Richmond Avenue, Brandon 10. Saskatchewan Avenue, Winnipeg "CAA Manitoba urges all levels of government to prioritize road safety through predictable, year-over-year investment and timely repairs," adds Friesen. “CAA Manitoba will continue to advocate for Manitobans to drive positive change in communities across the province." For more information and historical results, please visit: https://www.caamanitoba.com/advocacy/government-relations/worst-roads



Rural health documentary earns Peabody Award for Georgia Southern professor
Georgia Southern University Professor Matthew Hashiguchi has won a Peabody Award for his documentary, “The Only Doctor,” which focuses on rural health and the services provided by a single doctor in southwest Georgia. The Peabody Awards are prestigious accolades in storytelling across television, radio, streaming and other digital mediums. Categories for winning a Peabody include journalism, social video, interactive documentary, gaming and more. The nearly hour-long feature received the award in the Public Service category, which recognizes projects that address or respond to public health concerns, enhance public engagement or educate the public. For Hashiguchi, the award represents a personal and career accolade. “This award isn’t just a professional achievement, but also represents a moment in my life where I became a father,” said Hashiguchi. “I started filming right before my first daughter was born, and finished right after the second. While this award is an incredible acknowledgment of my work, it means even more to me as a priceless moment from their childhood.” The documentary focuses on Karen Kinsell, M.D., the sole physician serving 3,000 citizens in Clay County, Georgia, near the Georgia-Alabama border. The film spotlights the plight of a community in need of medical assistance and the dedicated doctor fighting to keep her clinic’s doors open. Hashiguchi delves into Kinsell’s sacrifices for her clinic’s operations, revealing her commitment to her patients. “Dr. Kinsell gets calls at home at all hours of the day and night,” Hashiguchi said. “She, at times, has had to pay the bills from her own bank account. But I’d say the biggest sacrifice is that she’s a doctor who does not have breaks.” The final cut of “The Only Doctor” is a bit different from the angle Hashiguchi took when he began work on it several years ago. He initially started the project to better understand the risks associated with maternal health care and childbirth when he and his wife were expecting their first child. Through his work, he learned of a more complex issue of health care access in rural communities. The documentary first premiered on the PBS program Reel South and is now available internationally on Al Jazeera’s documentary series “Witness.” Hashigchi’s work earned him a 2019 Gucci Tribeca Documentary Fund award and a 2021 American Stories Documentary Fund award from Points North Institute. The film’s world premiere took place at the 2023 Hot Docs International Documentary Film Festival in Toronto, Canada, and was awarded Best Documentary Feature at the 2024 South Georgia Film Festival, Best Feature at the 2023 Newburyport Documentary Film Festival and Award of Merit at the 2023 University Film and Video Association Conference. His rise to media prominence wasn’t on his radar early in his academic career. He described himself as a “C student,” and still sees himself as that young boy struggling with math and science courses. With one of the nation’s highest media honors, he can show his students new paths to success as well as the skills it takes to win a Peabody. “I want my students to know how I failed and know that I struggled,” he said. “I tell them that if they want to excel, they really have to put in hard work. That’s very much who I am now as I devote myself to these films.” If you're interested in learning more and want to book time to talk or interview with Matthew Hashiguchi then let us help - simply contact Georgia Southern's Director of Communications Jennifer Wise at jwise@georgiasouthern.edu to arrange an interview today.


Annual Healthy Georgia Report looks at public health in the Peach State
The fourth edition of the “Healthy Georgia: Our State of Public Health” report has been released by the Institute of Public and Preventive Health in Augusta University’s School of Public Health. Within the 64 pages of the report is a snapshot of how healthy Georgians are compared to citizens across the 12 states that make up the Southeastern Region (Alabama, Arkansas, Florida, Georgia, Kentucky, Louisiana, Mississippi, North Carolina, South Carolina, Tennessee, Virginia and West Virginia) and the entire United States. The 2025 edition addresses 31 health topics and has been expanded this year to include multimorbidity; long COVID-19; HIV, chlamydia, gonorrhea and syphilis infection rates; opioid and methamphetamine drug use; suicides; and vaping. Biplab Datta, PhD, assistant professor in the Department of Health Management, Economics, and Policy in SPH, heads up the team of IPPH faculty and staff who create the report each year. Datta credits Jen Jaremski, research associate, and Kit Wooten, public health analyst, with handling much of the work of bringing the report to life. Together, Jaremski and Wooten collected and organized all of the needed assets and organized the 64-page document, preparing it for print and the web. “Every year we strive to present data in a way that policymakers may find helpful in making policy choices,” Datta said. “There are several new topics that were added to this year’s report and some of those are concerning for the state of Georgia, particularly the communicable diseases like HIV, chlamydia, gonorrhea and syphilis. High prevalence rates of these conditions in Georgia, compared to the rest of the U.S. and the Southeastern Region, warrant attention of the public health community.” Georgia has the second-highest rate of HIV infections in the U.S., fourth-highest rates of gonorrhea, sixth-highest for chlamydia and 13th for syphilis. Something that is also new in this year’s report is a comparison of numbers from 2019, or before the COVID-19 pandemic began, compared to after the pandemic for certain conditions. Also coming out of the pandemic, the report looks at how long COVID has affected Georgians, with the state ranking 24th in the nation for rates of long COVID. According to the U.S. Centers for Disease Control and Prevention, long COVID is defined as a chronic condition that occurs after COVID-19 infection and is present for at least three months. On top of looking at comparisons between Georgia and the Southeast and the nation, Datta noted a clearer picture is starting to emerge concerning the difference in urban and rural areas within the state. “For several chronic conditions, like hypertension, diabetes and multimorbidity, we clearly see a striking difference between rural and urban residents of Georgia,” Datta said. Hypertension affects 44.1% of adults in rural Georgia compared to 35% in urban areas, while diabetes affects 17.5% of adults in rural Georgia compared to 12.3% of those in urban areas. Hypertension and diabetes are major risk factors for cardiovascular disease, which affects 12.2% of adults in rural areas compared to 8.3% of adults in urban areas of Georgia. “Hypertension and diabetes are the major risk factors for heart disease, which is the leading cause of death in the U.S. and worldwide, so these are some concerning numbers to see,” Datta said. Multimorbidity, which is when a person has multiple chronic conditions, including obesity, asthma, chronic obstructive pulmonary disease, depression, kidney disease, diabetes, hypertension, high cholesterol, cardiovascular disease, cancer, skin cancer and arthritis, affects 57.4% of adults in rural Georgia compared to 49% of adults in urban areas of the state. These rates are significantly lower than the rest of the Southeast but on par with the rest of the country. When comparing Georgia to the U.S. national average, adults in Georgia have lower rates of cancer and methamphetamine use but higher rates of childhood asthma and adult obesity. At the same time, rates of adult asthma and adult obesity among Georgians were comparable to the averages seen in the Southeast. Interestingly, while adult health insurance coverage was significantly lower than the U.S. national and Southeast Regional averages, the child health insurance coverage in Georgia was comparable to both national and regional averages. The Healthy Georgia Report is the only report of its kind in the state Looking to know more or connect with Biplab Datta, PhD? Then let us help. Dr. Datta is available to speak with media regarding this important topic. Simply click on his icon now to arrange an interview today.


Researchers at the Institute for Water and Health (IWH) at Georgia Southern University initiated a new project in Marion, Alabama, to address the city’s aging water infrastructure and its impact on human health with a focus on community-based research, workforce development and environmental justice. The pilot project in Marion, Alabama, is a collaborative effort between Georgia Southern and the University of Alabama. IWH Director Asli Aslan, Ph.D., is the principal investigator (PI) and Lacey Huffling, Ph.D., from Georgia Southern’s College of Education, and Lanna Nations, director for education and outreach for the Alabama Water Institute at the University of Alabama, are co-PIs. In partnership with the city of Eastman, Georgia, the project includes an internship program for next-generation water operators and a peer mentorship program for current water managers. Project leaders seek to improve communication and foster trust between local authorities and residents, contributing to long-term environmental health and equitable access to safe drinking water. Aslan sees workforce readiness as a critical component to maintaining standards in water management. “Nationwide, community water systems are managed by specialized professionals to ensure safe water every time we turn on the tap,” noted Aslan. According to her, about 50% of water operators working at these facilities will retire in the next decade, but only 10% are expected to be replaced. Training the next generation of water operators and developing leaders for rural water systems is a matter of national security. “The Institute for Water and Health is committed to launching a regional program to equip future water managers with the necessary skills to ensure safe water for all,” Aslan continued. “This pilot project will lay the foundation for this goal and aims to expand the program throughout the southeastern United States.” The project is funded by Alabama Power and Partnership for Inclusive Innovation, a Georgia-based program that funds and supports networks through resources across businesses, research universities and government entities. To learn more about this project and other IWH research and educational programs visit here. To connect with IWH Director Asli Aslan, simply click on her icon now to arrange an invterview today.


Exploring language as an early behavioral marker of Alzheimer's Disease
Professors from the University of Delaware and Carnegie Mellon University will use a $3.7 million RF1 grant from the National Institute on Aging (NIA) to examine language as an early behavioral marker of Alzheimer’s Disease. If successful, this research could pave the way for earlier interventions. “Identifying these individuals as early as possible gets them into preventive treatments sooner,” said Alyssa Lanzi, assistant professor of Communications Sciences & Disorders at UD. The study builds on pilot data gathered by Anna Saylor, a third-year doctoral student in the communication sciences and disorders doctoral program, housed in the UD's College of Health Sciences. “We know a lot about how language develops in childhood but not much about how it changes in older adults,” Saylor said. “Our data suggest subtle language changes might signal future cognitive decline.” To explore these changes on a larger scale, Lanzi is collaborating with MacWhinney, who founded TalkBank, open science database of language samples. Within TalkBank is DementiaBank, a shared database of multimedia interactions for studying communication in dementia. However, DementiaBank is outdated and limited in demographics, and the quality and rigor of the data need improvement. Lanzi is seeking to change that. Her five-year study seeks 300 older adults aged 60-90 nationwide from underrepresented backgrounds or populations vulnerable to health disparities. “Current DementiaBank data is representative of Caucasians of a higher socioeconomic status,” Lanzi said. “We must intentionally recruit people who are at the greatest risk — for example, adults who are Black, Asian, Hispanic, Latin and those living in rural areas.” The recruitment strategy, rooted in community engagement at locations in Wilmington, Delaware, is part of the novelty of Lanzi’s grant. “This is a feasibility study to see if our approach in Wilmington can be replicated in other states,” Lanzi said. Lanzi has also established an advisory committee of nationwide faculty with relevant expertise on specific priority populations. Their input will tailor plans to population needs while data is collected through a central site at UD. The Delaware Center for Cognitive Aging Research (DECCAR) also provides critical infrastructure for the study. “This project is an example of the success of DECCAR, and our impact extends far beyond state lines,” said Lanzi, an executive committee member with DECCAR. Participants selected for the study will participate in a comprehensive cognitive and language testing battery via telehealth, so they don’t have to travel to UD’s campus, which is novel and unique to this study. “To study their language, they’ll see pictures and be asked to describe them and share stories from their past,” Lanzi said. Study participants will receive a gift card for participating and feedback about their memory to share with their healthcare provider. “Building trust and giving back are key elements of our strategy,” Lanzi said. Lanzi is already preparing for the next phase of her research, supported by an additional $800,000 grant from the NIA. This phase will test the effects of an online treatment Lanzi developed for individuals identified as at risk. “If we find that language is an early marker of disease, I want to take this research to the next level and develop treatments that teach strategies to enhance independence and improve the quality of life for those at risk of developing dementia,” she said.


MEDIA RELEASE: Are you Ready for Winter Driving? CAA Manitoba shares winter weather readiness tips
As the cold weather begins to roll in, CAA Manitoba (CAA MB) is encouraging Manitobans to prepare themselves and their vehicles accordingly for the winter season. “All too often, motorists wait until the first snowfall before preparing their vehicles for winter driving,” says Nadia Matos, manager, external communications for CAA Manitoba. “Now is the time to get your winter tires on and check that your car battery will last the winter months. Even a fully charged battery can lose power when the temperature dips below 0° Celsius.” CAA Manitoba has compiled a list of winter readiness tips for Manitobans to help them prepare for the winter season. • Install winter tires for better traction – On cold and snowy roads winter tires can help reduce your breaking distance by up to 25 per cent. Members can call CAA before Nov. 30 to have our mobile tire service change them for you at home for a fee. • Test your car battery - If necessary, replace it before it fails. Even a fully charged battery can lose up to 30 per cent charge in temperatures below zero. CAA Manitoba will test Members’ batteries free of cost during a service call. • Ensure you have an emergency car kit – Your kit should have water, non-perishable food, jumper cables, blankets, a flashlight, batteries, waterproof matches, candles, and cat litter to help create traction under your tires. Add extra mitts, hats, socks and footwear to your emergency kit. • Have your brakes checked - If you’ve noticed any change in the feel of your brakes, or if they’re squealing or grinding, it may be time to have them serviced. With black ice and unpredictable weather, having good brakes can mean the difference between stopping and sliding. • Check your block heater- When you park– is your outdoor plug drawing power? Is your extension cord working with no missing prongs or exposed wires? • Check your lighting system - Make sure all your interior and exterior lights are working. For safe driving, ensure your headlights are aimed correctly. • Top up your fluids - Keep extra fluid in your trunk. Make sure it’s rated for -40ºC. Don’t let your gas drop below half full. • Inspect your wiper blade – Check the condition of your blades if you notice streaking on the windshield. Check for fraying or cracking and remove worn wiper blades and replace them with new ones. • Ensure you have the appropriate winter tools - Keep an ice scraper, small shovel and snow brush handy in your car at all times. While it’s important to make sure your vehicle is ready to go, it’s also important for drivers and passengers to be prepared in case of an emergency or if you are stranded. Some additional ways to be prepared include: Have a cell phone battery bank and keep it on you, as well as a charging cable that connects your phone to your vehicle. • Download and register for the CAA app and keep your CAA membership card in your wallet or vehicle so you always know how to contact CAA Manitoba if you are stranded. • Check Manitoba 511.ca for road conditions and closures if you head into a rural area. • Always tell your loved ones where you plan to go and what your route is before leaving on a longer trip in your vehicle. “Member safety is always our top priority at CAA Manitoba,” says Matos. “There’s no better time than the present to ensure you, your loved ones and your vehicle are ready to drive safely this winter season.” For more information about driving safely in winter conditions, please visit our Safe Winter Driving page at caamanitoba.com.


Expert Insight: Training Innovative AI to Provide Expert Guidance on Prescription Medications
A new wave of medications meant to treat Type II diabetes is grabbing headlines around the world for their ability to help people lose a significant amount of weight. They are called GLP-1 receptor agonists. By mimicking a glucagon-like peptide (GLP) naturally released by the body during digestion, they not only lower blood sugar but also slow digestion and increase the sense of fullness after eating. The two big names in GLP-1 agonists are Ozempic and Wegovy, and both are a form of semaglutide. Another medication, tirzepatide, is sold as Mounjaro and Zepbound. It is also a glucose-dependent insulinotropic polypeptide (GIP) agonist as well as GLP-1. Physicians have been prescribing semaglutide and tirzepatide with increasing frequency. However, both medications come with a host of side effects, including nausea and stomach pain, and are not suitable for every patient. Many clinics and physicians do not have immediate access to expert second opinions, as do the physicians at Emory Healthcare. Creating a Digital Twin That lack of an expert is one of the reasons Karl Kuhnert, professor in the practice of organization and management at Emory University’s Goizueta Business School, is using artificial intelligence to capture the expertise of physicians like Caroline Collins MD through the Tacit Object Modeler™, or TOM. By using TOM, developed by Merlynn Intelligence Technologies, Kuhnert and Collins can create her “decision-making digital twin.” This allows Collins to reveal her expertise as a primary care physician with Emory Healthcare and an Assistant Professor at Emory School of Medicine, where she has been leading the field in integrating lifestyle medicine into clinical practices and education. Traditional AI, like ChatGPT, uses massive amount of data points to predict outcomes using what’s known as explicit knowledge. But it isn’t necessarily learning as it goes. According to Kuhnert, TOM has been designed to learn how an expert, like Collins, decides whether or not to prescribe a drug like semaglutide to a patient. Wisdom or tacit knowledge is intuitive and rooted in experience and context. It is hard to communicate, and usually resides only in the expert’s mind. TOM’s ability to “peek into the expert’s mind makes it a compelling technology for accessing wisdom.” “Objective or explicit knowledge is known and can be shared with others,” says Kuhnert. "For example, ChatGPT uses explicit knowledge in its answers. It’s not creating something new. It may be new to you as you read it, but somebody, somewhere, before you, has created it. It’s understood as coming from some source." Karl Kuhnert “Tacit knowledge is subjective wisdom. Experts offer this, and we use their tacit know-how, their implicit knowledge, to make their decisions. If it were objective, everyone could do it. This is why we hire experts: They see things and know things others don’t; they see around corners.” Mimicking the Mind of a Medical Expert Teaching TOM to see around the corners requires Collins to work with the AI over the course of a few days. “Essentially what I do is I sit down with, in this case, a physician, and ask them, ‘What are thinking about when you make this decision?'” says Kuhnert. “The layperson might think that there are hundreds of variables in making a medical decision like this. With the expert’s tacit knowledge and experience, it is usually between seven and twelve variables. They decide based on these critical variables,” he says. "These experts have so much experience, they can cut away a lot of the noise around a decision and get right to the point and ask, ‘What am I looking at?’" Karl Kuhnert As TOM learns, it presents Collins with more and different scenarios for prescribing semaglutide. As she makes decisions, it remembers the variables present during her decision-making process. “Obviously, some variables are going to be more important than other variables. Certain combinations are going to be challenging,” says Collins. “Sometimes there are going to be some variables where I think, yes, this patient needs a GLP-1. Then there may be some variables where I think, no, this person really doesn’t need that. And which ones are going to win out? That’s really where TOM is valuable. It can say, okay, when in these difficult circumstances where there are conflicting variables, which one will ultimately be most important in making that decision?” The Process: Trusting AI After working with TOM for several hours, Collins will have reacted to enough scenarios for TOM to learn to make her decision. The Twin will need to demonstrate that it can replicate her decision-making with acceptable accuracy—high 90s to 100 percent. Once there, Collins’ Twin is ready to use. “I think it’s important to have concordance between what I would say in a situation and then what my digital twin would say in a situation because that’s our ultimate goal is to have an AI algorithm that can duplicate what my recommendation would be given these circumstances for a patient,” Collins says. “So, someone, whether that be an insurance company, or a patient themselves or another provider, would be able to consult TOM, and in essence, me, and say, in this scenario, would you prescribe a GLP-1 or not given this specific patient’s situation?” The patient’s current health and family history are critical when deciding whether or not to prescribe semaglutide. For example, according to Novo Nordisk, the makers of Ozempic, the drug should not be prescribed to patients with a history of problems with the pancreas or kidneys or with a family history of thyroid cancer. Those are just the start of a list of reasons why a patient may or may not be a good candidate for the medication. Kuhnert says, “What we’re learning is that there are so many primary care physicians right now that if you come in with a BMI over 25 and are prediabetic, you’re going to get (a prescription). But there’s much more data around this to suggest that there are people who are health marginalized, and they can’t do this. They should not have this (medication). It’s got to be distributed to people who can tolerate it and are safe.” Accessing the Digital Twin on TOM Collins’s digital twin could be available via something as easy to access as an iPhone app. “Part of my job is to provide the latest information to primary care physicians. Now, I can do this in a way that is very powerful for primary care physicians to go on their phones and put it in. It’s pretty remarkable, according to Colllins.” It is also transparent and importantly sourced information. Any physician using a digital twin created with TOM will know exactly whose expertise they are accessing, so anyone asking for a second opinion from Colllins will know they are using an expert physician from Emory University. In addition to patient safety, there are a number of ways TOM can be useful to the healthcare industry when prescribing medications like semaglutide. This includes interfacing with insurance companies and the prior approval process, often lengthy and handled by non-physician staff. “Why is a non-expert at an insurance company determining whether a patient needs a medication or not? Would it be better to have an expert?” says Collins. “I’m an expert in internal medicine and lifestyle medicine. So, I help people not only lose weight, but also help people change their behaviors to optimize their health. My take on GLP-1 medications is not that everyone needs them, it’s that they need to be utilized in a meaningful way, so patients will get benefit, given risks and benefits for these medications.” The Power of a Second Opinion Getting second, and sometimes third, opinions is a common practice among physicians and patients both. When a patient presents symptoms to their primary care physician, that physician may have studied the possible disease in school but isn’t necessarily an expert. In a community like Emory Healthcare, the experts are readily available, like Collins. She often serves as a second opinion for her colleagues and others around the country. “What we’re providing folks is more of a second opinion. Because we want this actually to work alongside someone, you can look at this opinion that this expert gave, and now, based on sourced information, you can choose. This person may be one of the best in the country, if not the world, in making this decision. But we’re not replacing people here. We’re not dislocating people with this technology. We need people. We need today’s and tomorrow’s experts as well,” according to Kuhnert. But also, you now have the ability to take an Emory physician’s diagnosing capabilities to physicians in rural areas and make use of this information, this knowledge, this decision, and how they make this decision. We have people here that could really help these small hospitals across the country. Caroline Collin MD Rural Americans have significant health disparities when compared to those living in urban centers. They are more likely to die from heart disease, cancer, injury, chronic respiratory disease, and stroke. Rural areas are finding primary care physicians in short supply, and patients in rural areas are 64 percent less likely to have access to medical specialists for needed referrals. Smaller communities might not have immediate access to experts like a rheumatologist, for example. In addition, patients in more rural areas might not have the means of transportation to get to a specialist, nor have the financial means to pay for specialized visits for a diagnosis. Collins posits that internal medicine generalists might suspect a diagnosis but want to confirm before prescribing a course of treatment. “If I have a patient for whom I am trying to answer a specific question, ‘Does this patient have lupus?’, for instance. I’m not going to be able to diagnose this person with lupus. I can suspect it, but I’m going to ask a rheumatologist. Let’s say I’m in a community where unfortunately, we don’t have a rheumatologist. The patient can’t see a rheumatologist. That’s a real scenario that’s happening in the United States right now. But now I can ask the digital twin acting as a rheumatologist, given these variables, ‘Does this patient have lupus?’ And the digital twin could give me a second opinion.” Sometimes, those experts are incredibly busy and might not have the physical availability for a full consult. In this case, someone could use TOM to create the digital twin of that expert. This allows them to give advice and second opinions to a wider range of fellow physicians. As Kuhnert says, TOM is not designed or intended to be a substitute for a physician. It should only work alongside one. Collins agreed, saying, “This doesn’t take the place of a provider in actual clinical decision-making. That’s where I think someone could use it inappropriately and could get patients into trouble. You still have to have a person there with clinical decision-making capacity to take on additional variables that TOM can’t yet do. And so that’s why it’s a second opinion.” “We’re not there yet in AI says Collins. We have to be really careful about having AI make actual medical decisions for people without someone there to say, ‘Wait a minute, does this make sense?’” AI Implications in the Classroom and Beyond Because organizations use TOM to create digital twins of their experts, the public cannot use the twins to shop for willing doctors. “We don’t want gaming the system,” says Collins. “We don’t want doctor shopping. What we want is a person there who can utilize AI in a meaningful way – not in a dangerous way. I think we’ll eventually get there where we can have AI making clinical decisions. But I don’t think I’d feel comfortable with that yet.” The implications of using decision-making digital twins in healthcare reach far beyond a second opinion for prescription drugs. Kuhnert sees it as an integral part of the future of medical school classrooms at Emory. In the past, teaching case studies have come from books, journals, and papers. Now, they could come alive in the classroom with AI simulation programs like TOM. "I think this would be great for teaching residents. Imagine that we could create a simulation and put this in a classroom, have (the students) do the simulation, and then have the physician come in and talk about how she makes her decisions." Karl Kuhnert “And then these residents could take this decision, and now it’s theirs. They can keep it with them. It would be awesome to have a library of critical health decisions made in Emory hospitals,” Kuhnert says. Collins agreed. “We do a lot of case teaching in the medical school. I teach both residents and medical students at Emory School of Medicine. This would be a really great tool to say, okay, given these set of circumstances, what decision would you make for this patient? Then, you could see what the expert’s decision would have been. That could be a great way to see if you are actually in lockstep with the decision-making process that you’re supposed to be learning.” Kuhnert sees decision-making twins moving beyond the healthcare system and into other arenas like the courtroom, public safety, and financial industries and has been working with other experts to digitize their knowledge in those fields. "The way to think about this is: say there is a subjective decision that gets made that has significant ramifications for that company and maybe for the community. What would it mean if I could digitize experts and make it available to other people who need an expert or an expert’s decision-making?" Karl Kuhnert “You think about how many people aren’t available. Maybe you have a physician who’s not available. You have executives who are not available. Often expertise resides in the minds of just a few people in an organization,” says Kuhnert. “Pursuing the use of technologies like TOM takes the concept of the digital human expert from simple task automation to subjective human decision-making support and will expand the idea of a digital expert into something beyond our current capabilities,” Kuhnert says. “I wanted to show that we could digitize very subjective decisions in such areas as ethical and clinical decision-making. In the near future, we will all learn from the wisdom codified in decision-making digital twins. Why not learn from the best? There is a lot of good work to do.” Karl Kuhnert is a Professor in the Practice of Organization & Management and Associate Professor of Psychiatry, School of Medicine and Senior Faculty Fellow of the Emory Ethics Center. If you're looking to connect with Karl to know more - simply click on his icon now to arrange a time to talk today.

