Experts Matter. Find Yours.
Connect for media, speaking, professional opportunities & more.

Hats off to the 2,100 graduates at Georgia Southern
Last week, approximately 2,100 undergraduate and graduate students from Georgia Southern University’s Statesboro, Armstrong and Liberty campuses received associate, baccalaureate, master’s, specialist and doctoral degrees in three Fall 2021 Commencement ceremonies. Georgia Southern President Kyle Marrero welcomed the graduates and their families to the University’s Fall Commencement ceremonies, held at the Savannah Convention Center in Savannah on Dec. 11, and the Allen E. Paulson Stadium in Statesboro on Dec. 13 and 14. He commended the graduates on their achievements and tenacity. “Graduates, I don’t need to tell you about your unique college journey, which has been challenging for all of us,” said Marrero. “I am very proud of how, together, we have persevered allowing us to have a successful semester and today, our commencement ceremony. You, our graduates, deserve great recognition.” During the Savannah ceremony, Georgia’s 2022 Teacher of the Year Cherie Dennis (Armstrong ‘10), who teaches English to Speakers of Other Languages at Hesse K-8 School in Savannah-Chatham County Public Schools, addressed the packed house with a call for kindness. “My hope for you is that you go out into the world with your eyes and your hearts wide open,” she said. “That you go out into the world and make something beautiful out of its cracks and imperfections. A world that is bound together by the irrefutable strength and integrity of kindness. Be the repairers of the world; the menders of the world; the bridge builders; the constructive, contributive citizens who nurture communities large and small. And that may sound daunting, but really it all starts with something so very simple, something so very possible and within your reach. Something you knew how to do even as a child. Just being kind.” Sachin Shailendra, chair of the University System of Georgia Board of Regents and president of SG Contracting, Inc. in Atlanta, spoke at the first ceremony in Statesboro. “Georgia Southern – which in a few minutes will be your alma mater – is one of the shining stars among our 26 institutions,” he said. “It ranks as one of Georgia’s best comprehensive universities, with a growing reputation for research that impacts not only vital industries but the environment and our communities. The degree you earned lets everyone know you learned from outstanding faculty, top staff and talented fellow students. “The opportunities ahead of you are many. I know this because of my own experience. I was born in Georgia, but my father was not. I am only a generation away from the farmers my family were in India. Education has been a game changer for both me and my family, and I know it’s a major accomplishment for many of you. I hope your degree will inspire you to take the next steps in building your future. So go out into the world and create a worthy future, not only for yourselves, but one that will represent Georgia Southern, our entire university system, and this state as well…Your education has already changed you. It also has the power to change your community, and move our state forward in exciting ways.” To read the full release please see the attachment below. This is a great moment for Georgia Southern University and if you are looking to learn more about this year's graduating class or the school - then let us help. Simply reach out to Georgia Southern Director of Communications Jennifer Wise at jwise@georgiasouthern.edu with your questions or to arrange an interview today.

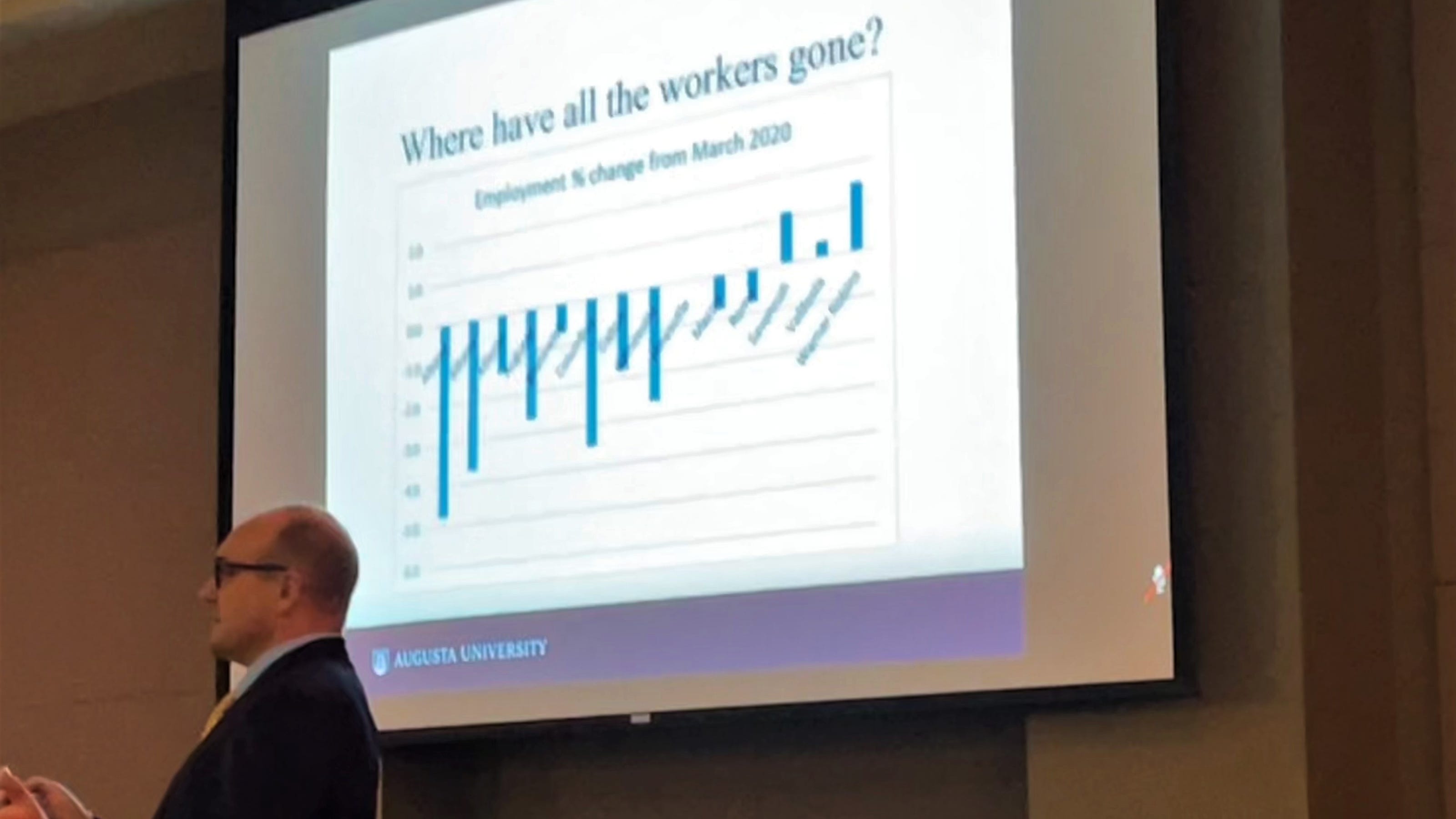
As the legendary political guru James Carville used to say, "It’s the economy, stupid." And these days with housing prices, inflation and the cost of living all pointing up in a very steep trajectory – the state of the economy is front and center for a lot of politicians, Americans and families as the year comes to a close. There’s a lot to be considered, and that’s where experts like Augusta’s Dr. Simon Medcalfe are being sought out to explain economic trends what is behind them. “U.S. retail sales are high,” explains Medcalfe “We had a lot of stimulus checks coming through the door and that’s really spurred extra spending and it’s across a whole range of retail sectors.” According to Medcalfe, household items are also seeing double-digit price increases. “What we’ve seen over the last 18 months during the pandemic, is a shift in our consumer preferences and consumer behavior.” • Furniture sales are up 29% • Used cars and cars in general are up 25-26% • Gardening and building supplies are up 14% • Electronics have seen an almost 30% increase • Clothing sales are up a whopping 50% But it’s not all good news - as the price of everything as we know is going up. “Inflation is running about 6.8% nationally,” Medcalfe explains. “It’s running about 7.2% in the south and it’s certainly a concern of policymakers and economists.” But theirs is sunshine behind those clouds as Medcalfe believes 2022 will see a return to normal. “I think next year inflation will come down. I know it won’t be at these high levels, but I still think it’ll be above the Feds target level of inflation, so look for those interest rate increases next year.” The economy and what to expect locally and nationally are hot topics – and if you are a reporter covering this topic – that’s where we can help. Dr. Simon Medcalfe is a highly regarded economics expert and the Cree Walker Chair in the Hull College of Business at Augusta University. Medcalfe is available to speak with media regarding the economy and its outlook – simply click on his icon now to arrange an interview today.


.jpg)
Is there such a thing as ‘a little cheating’ in American schools? Let our expert explain.
Cheating … it’s a universal tactic that seems to be a part of every academic institution regardless of subject, program or geography. Recently, Inside Higher Ed took a look at how students view cheating – and how their perspective of just what constitutes cheating is viewed. UMW’s David Rettinger provided his expert take on just what is going on in American schools. How acceptable is it to use study websites, or Google, to find answers to test or homework questions? What about using unapproved technology or tools to assist in an online exam? And would it be OK to give credit to another team member on a group project even if that person did not participate? These are a few ways the latest Student Voice survey, conducted in mid- to late October by Inside Higher Ed and College Pulse with support from Kaplan, explored the nuances of academic integrity and what students view as unethical… When David Rettinger, president emeritus of the International Center for Academic Integrity (ICAI), looked over the Student Voice data, he was drawn to the numbers that showed how much students realize certain actions would be considered cheating. “Some of [the unacceptable responses] are a little lighter for sure, but students generally would describe these behaviors as unacceptable,” says Rettinger, a professor of psychological science and director of academic integrity programs at the University of Mary Washington. “Their institutions talk about these things, and students know what they’re supposed to do, yet students cheat a fair bit.” He can imagine a stressed-out student saying, “I know it’s unacceptable, mostly I don’t do it, but in this situation, I’m going to do something I generally don’t believe in.” “That poses a problem for us as administrators,” he adds. December 07 – Inside Higher Ed Professor of Psychological Science David Rettinger oversees Academic Integrity Programs at the University of Mary Washington. He is available to provide expert insight into this study and the concept of students who cheat while attending at American colleges and universities. Simply click on his icon now to arrange an interview today.


Aston University pharmacy graduate honoured for charity fundraising work
An Aston University pharmacy graduate has been recognised for his charitable fundraising in the Chemist and Druggist Awards 2021. Shoaib Hussain managed to raise thousands of pounds within just four weeks when he shared a video detailing his 2017 trip to help at Rohingya refugee camps in Bangladesh. He received the Above and Beyond Award at a ceremony held at the InterContinental London – The O2 on 19 November. Shoaib’s powerful video resonated so strongly with the public that he smashed his £25,000 fundraising target in just 24 hours. His campaign eventually raised £135,000 – all of which was donated to the charity Global Helping Hands, which is run by UK medical professionals. The money has paid for thousands of survival packs and the building of a medical centre, over 100 homes, 30 wells, and seven educational sites in Mosques. Shoaib said: “The video shared a personal account and was extremely difficult for me to voice. It detailed something I have not even spoken to my wife about fully, and something I still cannot talk about without tearing up when I remember what I witnessed.” Shoaib dedicated his award to “the refugees who I helped, and the donors who made it possible”.


Head of School of Optometry named world expert in contact lenses
Professor James Wolffsohn, head of the School of Optometry at Aston University has been named by Expertscape as a world expert in contact lenses research based on his publications. Expertscape's PubMed-based algorithms placed professor Wolffsohn in the top 0.1 per cent of scholars writing about contact lenses over the past 10 years. He is also ranked by the same organisation as a world expert in presbyopia (the loss of eye focus with age affecting near vision), and is one of the top three scholars in the world. Expertscape is designed to help find the most knowledgeable physicians and health professionals in the world. Expertscape objectively ranks people and institutions by their expertise in more than 27,000 biomedical topics. James’ research focuses of the development, enhancement and validation of ophthalmic instrumentation to optimise contact lens comfort and fitting. He is also pioneering the use of contact lenses as a treatment for dry eyes; and developing methods to restore more natural eye focus through intraocular lenses, that are implanted into the eye as part of cataract surgery; as well as pharmaceutical approaches. Professor James Wolffsohn said: “I am delighted that our research in the field of contact lenses and presbyopia has had the desired impact and is widely read and cited. “Working together with colleagues in industry, we are able to accelerate product innovation, development and validation, leading to enhanced quality of life in patients.” James has published over 280 peer reviewed academic papers and given numerous international presentations. His main research areas are the development and evaluation of ophthalmic instrumentation, contact lenses, intraocular lenses and the tear film. A contact lens is a corrective, cosmetic, or therapeutic lens usually placed on the cornea of the eye. Contact lenses usually serve the same corrective purpose as conventional glasses, but are lightweight and virtually invisible. It has been estimated that about 125 million people use contact lenses worldwide. Presbyopia is the loss of eye focus with age which is usually noticed by ~45 years of age when reading glasses or another form of refractive correction is needed. It has a marked emotional effect being one of the first apparent signs of ageing.

UConn expert weighs in on controversial statue debate at the Connecticut Capitol
What should be the fate of the large statue commemorating John Mason that adorns the Connecticut State Capitol Building? He’s a historic figure and founder of the Connecticut Colony. He also left a legacy of violence and murder, with more than 400 Indigenous people, including 175 women and children, killed under his command. And whether to let his statue stand or remove it has engaged a debate from leading experts, historians, relatives of Mason, and the Indigenous community across the state. UConn’s Manisha Sinha was asked to lend her expertise to the situation: Manisha Sinha, a University of Connecticut professor of 19th century U.S. history, said she is a veteran of debates about the fate of statues memorializing Confederate leaders as well as founding fathers who owned slaves. “I have advocated for the taking down of statues that commemorate Confederate leaders and generals, who I see as traitors to the American republic, fighting for the worst cause in American history, as General Grant put it, in the cause of human bondage,” Sinha said. “On the other hand, I have opposed the taking down of statues of some of our founding fathers, revolutionary figures who did not defend slavery as a positive good.” Sinha said history can be complex, and great men of history can be flawed. “The Mason massacre is not a complex story,” she said. “It was a sheer massacre of non-combatants and of women, children and elders. We cannot excuse this by pointing to internecine warfare among Native Americans.” Mason’s statue is not necessary to teach history, she said. “I think it is high time that you think of removing John Mason’s statue,” Sinha said. “It cannot be contextualized. We do not remember history by statues, especially not in the monumental 19th century forms. We actually end up commemorating people, making them heroic.” November 18 – The CT Mirror This is a sensitive and very important topic as America reconciles with its past and moves forward as a country. And, if you are a journalist covering this topic, then let our experts help with your in-depth coverage and questions. Manisha Sinha is the Draper Chair in American History at the University of Connecticut and the author of "The Slave's Cause: A History of Abolition." She is an expert in the era of America during the 19th Century and available to speak with media regarding this topic – simply click on her icon now to arrange an interview today.



'Tangled Up' reveals science and history of Alzheimer's
A new book from leading University of East Anglia dementia expert Prof Michael Hornberger investigates the science and history of Alzheimer's disease. 'Tangled Up - The science and history of Alzheimer's disease' is available as a paperback or e-book. Prof Hornberger researches groups that are at higher risk of developing dementia (because of genetics, lifestyle or their other health condition) and works to help reduce this risk or delay the symptoms of dementia. He also explores the nature of support for those who have been diagnosed with dementia and helping the patients and their families and carers prepare for the future. His background is as a neuroscientist and his work involves using innovative techniques (such as online games and driver behaviour) to identify the spatial or navigation issues that can occur long before before diagnosis of dementia and before the traditional impacts on memory arise. He developed the mobile game Sea Hero Quest that can detect people at risk of Alzheimer's. His work enables early prediction of the likelihood of dementia (sometimes a decade ahead) and the opportunity to manage the onset and reduce risk by as much as 30 per cent. Prof Michael Hornberger, from UEA’s Norwich Medical School, said: “Alzheimer's disease is the most common cause of dementia in the UK. It affects around one in 14 people over the age of 65 and one in every six people over the age or 80 – and it can affect memory, thinking skills and other mental abilities. “I wanted to write a book to help people better understand the science and history of Alzheimer’s disease. “It covers everything from the causes of Alzheimer’s, through to why people with Alzheimer’s ‘live in the past’ and practical advice for how people can reduce the risk of developing it. “At the end of the book, you will have become an Alzheimer’s disease science expert and can use your newfound knowledge to untangle this devastating disease,” he added.


The Case for Career Advocates: An Organization Is Not a Meritocracy
“This blog post is the first in a three-part series that summarizes the key messages I deliver to my students, in the hopes that it can catalyze and support the career success of a broader group of ambitious employees who aspire to make it to the C-Suite,” writes Renee Dye 94PhD, associate professor in the practice of Organization & Management. “Most of my lessons are derived from my own unlikely personal journey from literary scholar to top-tier management consultant to C-suite executive for a publicly traded company, but they are also heavily informed by leading researchers like Sylvia Anne Hewlett. In the final blog, I discuss the impact of remote work on career success.” One of the paradoxes of the Gen-Zs and Generation Alphas is their intuitive understanding of the phenomenon of social media…at the same time they maintain an almost ideological conviction that the workplace – apart from systemic biases – is otherwise a meritocracy, where talent is perfectly and objectively evaluated – and the best and most deserving rise to the top. Surely a cursory exploration of Instagram and TikTok would convince even the most skeptical of the fundamentally idiosyncratic nature of success in a networked world? The Real World is likewise characterized by outcomes in which success is imperfectly correlated with capability level. Someone whose capability level is less than yours may lap you in the race to the top of the organization. That may seem unfair, but that’s because you’re making the mistake of assuming that career success is predicated purely on capability. A survey of MBA graduates from my school a few years ago produced a startling insight: of all the skills that we provided to our students during their MBA tenures, our students felt most unprepared to navigate “organizational politics” in their careers. The reason that I found this fact so astonishing is that today’s students, who are Digital Natives and in part Social Media Natives, are the most connected and self-promoting generation the world has ever seen. Yet today I find that my students continue to exhibit little practical understanding of how career success is forged…so much so that I now devote an entire class session in my core Strategy class to demonstrating the importance of relationship management and advocacy cultivation. Capability is not unimportant; far from it. As I tell my students, though, capability is table stakes these days as the level of education and skill sets continues to advance among individuals. If you’re not smart and capable you’re not getting in the door. But once you’re in, your career path and ultimate career success will be more determined by (1) your level of aspiration and unflagging commitment to achieving your goals; (2) your performance outcomes in your individual roles; (3) your work ethic and conscientiousness; and (4) the relationships you have with other people within your organization. And the relationships that matter the most are the individuals with influence and power over your future career opportunities. Let me put it starkly: without career advocates (notice the plural), it will be much, much harder to make it to the senior management ranks. Full stop. Some facts to bear this assertion out: • People with advocates are 23% more likely to move up in the careers • Women with advocates are 22% more likely to ask for a stretch assignment to build their reputations as leaders Ultimately, having an advocate confers a career benefit of 22-30%, depending on who’s doing the asking and what they’re asking for. That’s increasing your odds of making it to the C-Suite by nearly a third! If anecdotal evidence is more your thing, here are a couple of quotations for you: • A lot of decisions are made when you are not in the room, so you need someone to advocate for you, bring up the important reasons you should advance” (Catalyst Survey, as quoted in Elizabeth McDaid, “Mentor vs. Sponsor,” September 3, 2019) • When you get to the level in your career when decisions are not just being made by an individual manager, feedback from other leaders becomes crucial. Rosalind Hudnell, Chief Diversity Officer, Intel. As quoted in Hewlett, Sylvia Ann, Melinda Marshall, and Laura Sherbin. “The Relationship You Need to Get Right,” HBR 2011) • “I was great at building businesses and had tons of cheerleaders, but I had that typical Asian keep-your-head-down-and-you’ll-get-taken-care-of mindset.” My boss had to take me aside and tell me that if I didn’t actively cultivate her as my sponsor, I would never progress beyond senior associate” (quoted in Hewlett, Sylvia Ann, Melinda Marshall, and Laura Sherbin. “The Relationship You Need to Get Right,” HBR 2011) To reiterate: an organization is not purely a meritocracy where talent and hard work speak for themselves; and it’s much, much harder to advance within an organization without effective advocates. Renee Dye is an Professor in the Practice of Organization & Management at Goizueta Business School. For more insight and to continue reading this article and series, please visit Dye’s blog. To arrange an interview – simply click on Dye’s icon now to book a time today.



Aston University makes experts available through COP26
The University’s website is highlighting its experts, projects and research, latest news and podcasts around sustainability On 4 November the University’s Supergen Hub will co-host a ‘fishbowl’ conversation to develop and interrogate visions for a net zero energy future Aston Originals has produced three shows around finance, energy and transport ahead of the summit. Aston University has launched its COP26 campaign to highlight the work being done by its academics and researchers to support the United Nation’s biggest climate change targets. The University’s website will highlight its experts, projects and research, latest news and podcasts around sustainability and climate change. The COP26 summit will be attended by the countries that signed the United Nations Framework Convention on Climate Change (UNFCCC) – a treaty that came into force in 1994. More than 190 world leaders will meet in Glasgow, between 31 October and 12 November, to discuss ways of achieving net-zero carbon emissions by 2050 and keeping the global temperature rise to 1.5 degrees Celsius this century. High profile attendees are expected to include Greta Thunberg, Pope Francis and Sir David Attenborough. Representatives from Aston University will also be taking part at the global summit. On 4 November during ‘Energy Day’, the six UK Research and Innovation Supergen Hubs, one of which involves academics from Aston University, are hosting a ‘fishbowl’ conversation with the public, to develop and interrogate visions for a net zero energy future. It will be participant-driven, enabling multiple perspectives to be aired and offering an opportunity for a variety of participants to engage, and will be live-streamed for those who cannot attend in-person (tickets available for the live-stream here). Also during Energy Day at COP26, the Aston University Supergen Bioenergy Hub will be hosting a ‘Build your own biorefinery’ game on the COP26 Universities Network exhibition stand within the Green Zone. Members of the public will be invited to create their own biorefinery (where multiple products are created from one feedstock to extract maximum value), demonstrating the many routes to producing bioenergy and bioproducts and the co-benefits that can be achieved through different choices. The campaign will also look at the huge carbon footprint of asthma inhalers and a new project which aims to redesign the canisters, so they are more environmentally friendly. The University’s new digital content brand, Aston Originals, has produced three videos showcasing its experts under the topics of finance, energy and transport. Professor Simon Green, pro-vice chancellor research at Aston University, said: "COP26 highlights how big a challenge the climate crisis is for everyone around the world. “I am proud of the work being done at Aston University to combat the problems facing the planet – from the researchers in the College of Engineering and Physical Sciences carrying out world-leading research into new and innovative ways of converting biomass into sources of sustainable energy to experts in the College of Business and Social Sciences who are helping small and medium sized enterprises (SMEs) cut their carbon footprint.”

ChristianaCare Named a “Most Wired” Health Care Technology Leader for 6th Consecutive Year
ChristianaCare Recognized as one of the Nation’s Best in Both Ambulatory and Hospital Care (WILMINGTON, Del. – Oct. 29, 2021) For the sixth consecutive year, ChristianaCare has earned the “Most Wired” designation from the College of Healthcare Information Management Executives (CHIME), which assesses how effectively health care organizations apply core and advanced technologies to improve health and care in their communities. ChristianaCare was recognized with a Performance Excellence Award for Most Wired’s acute and ambulatory categories. That level is reserved only for organizations that are considered leaders in health care technology who “actively push the industry forward.” The recognition affirms that not only has ChristianaCare implemented advanced technologies, but it leverages those technologies in innovative ways. And it also has encouraged deep adoption of these technologies across the entire health system. “Throughout the COVID-19 pandemic, patients and providers have experienced the power of virtual care and the ability for data and technology to improve the health care experience,” said ChristianaCare President and CEO Janice E. Nevin, M.D., MPH. “At ChristianaCare, we believe now is the moment to transform our health care system to a new model of care that doesn’t stop between appointments—it’s continuous, data-driven and technology-enabled. We’re proud to be recognized as a leader in health care innovation, as we work to achieve better health at lower costs.” “We are driving digital into the core of our existing operations and simultaneously creating new digital product offerings,” said Randy Gaboriault, MS, MBA, chief digital and information officer at ChristianaCare. “The concept of the visit as the primary point of interaction between patient and doctor is obsolete. Our unique care foundation is continuous, digital and in the home, driving care with data and producing engagement actions between the visits. Our goal is for the care team, supported by artificial intelligence within the workflow, to determine the next best action for each patient.” The recognition is the latest accolade that highlights ChristianaCare’s success in creating exceptional experiences for its patients and consumers through personalized, proactive communication, which enables people to use the channels that they prefer in order to easily access care. This success was recently illustrated through ChristianaCare’s integration of clinical data with its new customer relationship management (CRM) system, which enabled ChristianaCare to scale and automate outreach to patients due for important preventive health checks. Through this effort and the new capabilities, ChristianaCare initiated patient and consumer outreach to address two common gaps in care – annual wellness checkups and breast cancer screenings. Continuous and automatic, the outreach within weeks resolved 11% of the gaps in annual wellness checkups, and 8% of the gaps in breast cancer screenings. “Success here stems from our commitment to continuously look for opportunities to innovate, from which we can more quickly and effectively partner with each individual on their path toward optimal health, even as we explore new ways to push the boundaries of how technology can further improve the health of our community,” said Lynne McCone, vice president of IT Application Services at ChristianaCare. The 2021 Digital Health Most Wired program assessed the adoption, integration and impact of technologies in health care organizations at all stages of development, from early development to industry-leading. Each participating organization received a customized benchmarking report, an overall score and scores for individual levels in eight segments: infrastructure; security; business/disaster recovery; administrative/supply chain; analytics/data management; interoperability/population health; patient engagement; and clinical quality/safety. Participants can use the report and scores to identify strengths and opportunities for improvement. Participants also received certification based on their overall performance. “Digital transformation in healthcare has accelerated to an unprecedented level since 2020, and the next few years will bring a wave of innovation that empowers healthcare consumers and will astound the industry,” said CHIME President and CEO Russell P. Branzell. “The Digital Health Most Wired program recognizes the outstanding digital leaders who have paved the way for this imminent revolution in healthcare. Their trailblazing commitment to rapid transformation has set an example for the entire industry in how to pursue a leadership vision with determination, brilliant planning and courage to overcome all challenges.” About ChristianaCare Headquartered in Wilmington, Delaware, ChristianaCare is one of the country’s most dynamic health care organizations, centered on improving health outcomes, making high-quality care more accessible and lowering health care costs. ChristianaCare includes an extensive network of primary care and outpatient services, home health care, urgent care centers, three hospitals (1,299 beds), a freestanding emergency department, a Level I trauma center and a Level III neonatal intensive care unit, a comprehensive stroke center and regional centers of excellence in heart and vascular care, cancer care and women’s health. It also includes the pioneering Gene Editing Institute. ChristianaCare is nationally recognized as a great place to work, rated by Forbes as the 5th best health system to work for in the United States and by IDG Computerworld as one of the nation’s Best Places to Work in IT. ChristianaCare is rated by HealthGrades as one of America’s 50 Best Hospitals and continually ranked among the nation’s best by Newsweek and other national quality ratings. ChristianaCare is a nonprofit teaching health system with more than 260 residents and fellows. With its groundbreaking Center for Virtual Health and a focus on population health and value-based care, ChristianaCare is shaping the future of health care.

