Experts Matter. Find Yours.
Connect for media, speaking, professional opportunities & more.

ChristianaCare Plans to Build Health Campus in Georgetown, Delaware
At a time when there is uncertainty about the future of heath care in the U.S., ChristianaCare is doubling down on its investments to expand access to care in Delaware. As part of $865 million in new investments in Delaware over three years that ChristianaCare announced last July, ChristianaCare today submitted a Notice of Intent to the Delaware Health Resources Board to develop a new health campus in Georgetown. The proposed campus will bring more comprehensive care closer to home for residents of Sussex County, an area experiencing rapid population growth and long-standing gaps in access to essential health services. Designed to Meet the Needs of a Growing Community Similar to ChristianaCare’s West Grove Campus in southern Chester County, Pennsylvania, and its upcoming campuses in Springfield and Aston in Delaware County, the new campus will feature a health center offering primary care, specialty care, behavioral health and other outpatient services and a neighborhood hospital with eight emergency beds and eight inpatient beds. This facility is designed to make it easier for residents to receive timely, high-quality care in their own community. “Sussex county is home to a growing and aging population and is designated by the Health Resources & Services Administration (HRSA) as a Medically Underserved Area,” said Janice E. Nevin, M.D., MPH, president and CEO of ChristianaCare. “This new campus will help close gaps in access by bringing high-quality, equitable and more convenient care directly into the community that needs it most. Our goal is simple: ensure that every Delawarean can access the care they need, in the right place at the right time.” Expanding Access While Strengthening Regional Care This new ChristianaCare campus will add local outpatient care, emergency and inpatient care, creating a closer network of services connecting residents to advanced specialty care at ChristianaCare’s regional hospitals. ChristianaCare is partnering with Emerus Holdings, Inc. with respect to the neighborhood hospital component. Emerus is the nation’s leading developer of this care delivery model, partnering in the operation of more than 45 acute care facilities nationwide. This partnership reflects ChristianaCare’s commitment to bringing nationally recognized, high-quality care to Delaware. “We are proud to continue our partnership with ChristianaCare to bring sustainable, compassionate and high-quality health care to the residents of Sussex County,” said Vic Schmerbeck, CEO of Emerus Holdings Inc. “Together, we are building a next-generation model of care designed around the needs of the community—today and for the future.” The 42,000-square-foot Georgetown campus is expected to open in late 2028. The campus is planned for 20769 DuPont Boulevard in Georgetown. The campus is estimated to cost $65.1 million. Planning for Today’s Demand and Tomorrow’s Growth ChristianaCare already offers a range of services in Sussex County—including primary care, specialty care, virtual care and home health and hospice services. However, Sussex and Kent counties are projected to see an 8% population increase by 2030, with a significant rise in residents age 65 and older. As demand for emergency, primary and specialty care grows, this new campus is designed to make care more local, more connected and more responsive to community needs. In addition, ChristianaCare will continue to explore opportunities to expand access to care in other areas of Delaware, including in Kent County.

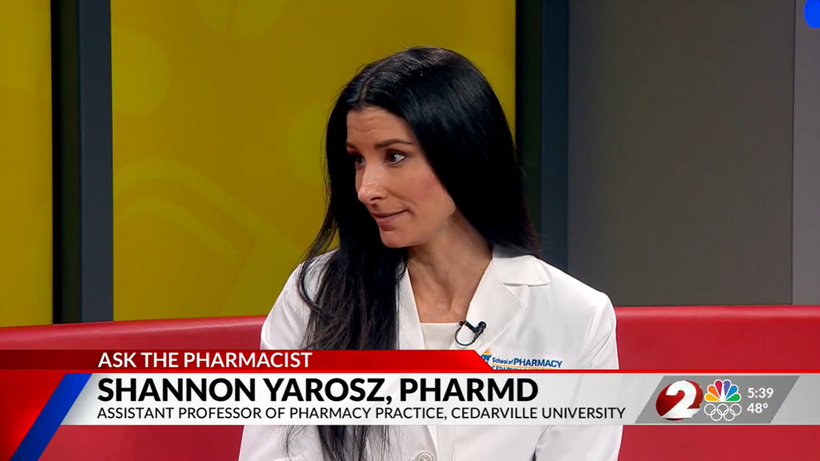
Experts in the Media: What You Need to Know About Medication Safety and Everyday Health
From medication safety to seasonal illness prevention, pharmacists are often the most accessible, and overlooked, healthcare professionals in our communities. In a recent segment on NBC, Dr. Shannon Yarosz breaks down common misconceptions about prescriptions, explains how drug interactions really work, and shares practical advice patients can use immediately to better manage their health. Dr. Shannon Yarosz is an Assistant Professor of Pharmacy Practice. Prior to joining the faculty at Cedarville University, served in multiple pharmacy roles. Her career reflects a deep commitment to patient care with experience in pediatrics, community pharmacy practice, and clinical healthcare services. As healthcare systems face growing pressure and patients navigate increasingly complex medication regimens, pharmacists are playing a larger role than ever before. This discussion highlights why their expertise matters, from helping patients avoid costly mistakes to providing front-line guidance on everyday health concerns. When should I stop taking antibiotics? Is it ok to stop when I begin feeling better? This question and several others were addressed in this week's Ask the Pharmacist segment on WDTN TV in Dayton, Ohio. Looking to know more or connect with Dr. Shannon Yarosz? Simply contact: Mark D. Weinstein Executive Director of Public Relations Cedarville University mweinstein@cedarville.edu


The Secret to Happiness? Feeling Loved.
After more than 50 years studying close relationships, University of Rochester psychologist Harry Reis has reached a deceptively simple conclusion: Happy people feel loved. That conclusion became the jumping-off point for a new book Reis co-wrote, “How to Feel Loved: The Five Mindsets That Get You More of What Matters Most” (Harper 2026), which blends decades of research on happiness and human connection. In it, Reis and his co-author, Sonja Lyubomirsky, a psychologist at the University of California, Riverside, outline five research-backed mindsets that strengthen connection: sharing authentically, listening to people, practicing radical curiosity, approaching others with an open heart, and recognizing human complexity. The book was recently featured in The New York Times, which noted that the authors contend giving and receiving love function together like a seesaw: You lift a person up with the weight of your curiosity and attentiveness — and they do the same in turn. “The other side is very important also,” Reis told The Times. “To be sharing what’s important to you, to be sharing what you’re concerned about, so it can really become a two-way street.” Reis, who leads groundbreaking research on close relationships, is available to discuss: • The science of feeling loved vs. being loved • How digital distraction undermines connection • AI companionship and its psychological limits • Practical ways to build stronger, more resilient relationships • The link between love, happiness, and health Journalists writing about love and relationships can contact Reis by clicking on his profile.



Scientist’s cat, again, helps discover new virus
Pepper, the pet cat who made headlines last year for his role in the discovery of the first jeilongvirus found in the U.S., is at it again. This time, his hunting prowess contributed to the identification of a new strain of orthoreovirus. John Lednicky, Ph.D., Pepper’s owner and a University of Florida College of Public Health and Health Professions virologist, took Pepper’s catch — a dead Everglades short-tailed shrew — into the lab for testing as part of his ongoing work to understand transmission of the mule deerpox virus. Testing revealed the shrew had a previously unidentified strain of orthoreovirus. Viruses in this genus are known to infect humans, white-tailed deer, bats and other mammals. While orthoreoviruses’ effects on humans are not yet well understood, there have been rare reports of the virus being associated with cases of encephalitis, meningitis and gastroenteritis in children. “The bottom line is we need to pay attention to orthoreoviruses, and know how to rapidly detect them,” said Lednicky, a research professor in the PHHP Department of Environmental and Global Health and a member of UF’s Emerging Pathogens Institute. The UF team published the complete genomic coding sequences for the virus they named “Gainesville shrew mammalian orthoreovirus type 3 strain UF-1” in the journal Microbiology Resource Announcements. “There are many different mammalian orthoreoviruses and not enough is known about this recently identified virus to be concerned,” said the paper’s lead author Emily DeRuyter, a UF Ph.D. candidate in One Health. “Mammalian orthoreoviruses were originally considered to be ‘orphan’ viruses, present in mammals including humans, but not associated with diseases. More recently, they have been implicated in respiratory, central nervous system and gastrointestinal diseases.” The Lednicky lab’s jeilongvirus and orthoreovirus discoveries come on the heels of the team publishing their discovery of two other novel viruses found in farmed white-tailed deer. Given the propensity of viruses to constantly evolve, paired with the team’s sophisticated lab techniques, finding new viruses isn’t entirely surprising, Lednicky said. “I’m not the first one to say this, but essentially, if you look, you’ll find, and that’s why we keep finding all these new viruses,” Lednicky said. Like influenza virus, two different types of orthoreovirus can infect a host cell, causing the viruses’ genes to mix and match, in essence, creating a brand new virus, Lednicky said. In 2019, Lednicky and colleagues isolated the first orthoreovirus found in a deer. That strain’s genes were nearly identical to an orthoreovirus found in farmed mink in China and a deathly ill lion in Japan. How in the world, the scientific community wondered, could the same hybrid virus appear in a farmed deer in Florida and two species of carnivores across the globe? Some experts speculated that components of the animals’ feed could have come from the same manufacturer. With so many unanswered questions about orthoreoviruses and their modes of transmission, prevalence in human and animal hosts and just how sick they could make us, more research is needed, DeRuyter and Lednicky said. Next steps would include serology and immunology studies to understand the threat Gainesville shrew mammalian orthoreovirus type 3 strain UF-1 may hold for humans, wildlife and pets. For readers concerned about Pepper’s health, rest assured. He has shown no signs of illness from his outdoor adventures and will likely continue to contribute to scientific discovery through specimen collection. “This was an opportunistic study,” Lednicky said. “If you come across a dead animal, why not test it instead of just burying it? There is a lot of information that can be gained.”



Epidemiologist: Winter Olympics fortunate to dodge norovirus outbreak
Finland's Olympic women's hockey team overcame a norovirus scare last week, but they couldn't get past Team USA, who shut them out 5-0 Saturday in Milan. The University of Delaware's Jennifer Horney can discuss the difficult-to-contain virus, which also hit the Winter Games in 2018. - Horney, a professor of epidemiology at UD, said that the outbreak – which forced Finland to cancel its first game after 13 players had either been infected or quarantined – is not surprising. Norovirus spreads rapidly in crowded environments through direct contact with surfaces or airborne droplets. - It is difficult to limit the spread of norovirus, as witnessed by the major outbreak that spread at the 2018 Winter Olympics in South Korea. - Consideration is often given for the potential of these types of outbreaks being intentional, which requires public health to work closely with law enforcement. To reach Horney directly and arrange an interview, visit her profile and click on the "contact" button. Interested journalists can also send an email to MediaRelations@udel.edu.



Most patients taking popular weight loss and diabetes medications such as Ozempic and Wegovy can safely continue them before gynecologic surgery, according to a new journal article from ChristianaCare published in Obstetrics & Gynecology. The review found that serious anesthesia risks linked to these drugs are uncommon for most patients and can usually be managed through individualized planning rather than stopping the medication. The paper is the first to take a focused look at glucagon-like peptide-1 receptor agonists, commonly called GLP-1 drugs, in gynecologic surgery. These medications were first approved to treat diabetes and are now widely used to support weight loss and metabolic health, which refers to how the body processes sugar and energy. “Our study shows that the evidence does not support routinely stopping these medications before surgery and that the actual risk is low for most patients,” said Michelle Pacis, M.D., MPH, senior author of the study and a minimally invasive gynecologic surgeon at ChristianaCare. Why these medications raised concerns GLP-1 drugs work in part by slowing how quickly the stomach empties. This helps patients feel full longer, but it also raises concerns for surgery. Doctors worry that food remaining in the stomach could increase the risk of aspiration, when stomach contents enter the lungs during anesthesia. Because of this, early recommendations often advised stopping GLP-1 medications before surgery. The ChristianaCare review found that this approach was largely based on caution rather than strong evidence. The authors reviewed data from multiple studies, including large patient groups, that examined outcomes in people taking GLP-1 drugs during procedures. While some studies showed higher amounts of stomach contents, aspiration events were rare and occurred at rates similar to patients who were not taking the medications. New guidance reflects a change in thinking Recent national guidance from several medical societies now recommends a more tailored approach. Most patients can continue GLP-1 medications before surgery. For patients with higher risk factors, such as significant stomach symptoms or known delayed digestion, simple precautions can reduce risk. These precautions may include a clear liquid diet for 24 hours before surgery or closer monitoring during anesthesia. A clear liquid diet includes fluids like water, broth and clear juices. “This shift recognizes both the benefits of these medications and the importance of patient-specific decision making,” Pacis said. Why this matters for gynecologic surgery Many gynecologic surgeries require patients to be positioned in ways that can affect breathing and circulation. At the same time, many patients needing these procedures also have obesity or diabetes, which can increase surgical risk. GLP-1 medications can improve blood sugar control and support weight loss, helping patients enter surgery in better overall health and enhance recovery. Stopping these drugs without a clear reason may work against those benefits. Practical steps to support patient safety The study outlines several strategies care teams can use when patients remain on GLP-1 medications. These include thoughtful anesthesia planning, careful monitoring of heart and lung function, and, in select cases, the use of ultrasound to check stomach contents before surgery. “The goal is not to ignore risk, but to manage it wisely,” Pacis said. “For many patients, continuing these medications supports safer surgery and better recovery.” The authors note that more research is needed, particularly studies focused specifically on gynecologic surgery. Still, the findings offer clarity for patients and clinicians navigating a rapidly changing area of care. “This review helps bring evidence and balance to an issue that has caused a lot of confusion,” Pacis said. “It supports keeping patients on therapies that benefit their health whenever it is safe to do so.”
ExpertSpotlight: The Surprising (and Slightly Dark) History of Valentine’s Day
Valentine’s Day may now be synonymous with chocolates, flowers, and heart-shaped everything, but its origins are far more complex, blending ancient Roman traditions, Christian martyrdom, and medieval storytelling. What began as a mid-winter festival tied to fertility and renewal eventually evolved into a celebration of romantic love - one shaped as much by poets and pop culture as by saints and religious history. Ancient Roots: Before Romance, There Was Ritual Long before Valentine’s cards, ancient Romans celebrated Lupercalia, a mid-February festival focused on fertility, purification, and the coming of spring. The event included symbolic rituals meant to ward off evil spirits and promote health and fertility, far removed from today’s candlelit dinners. As Christianity spread through the Roman Empire, many pagan festivals were re-interpreted or replaced with Christian observances, laying the groundwork for what would become Valentine’s Day. Who Was Valentine, Anyway? There isn’t just one Valentine. Historical records point to multiple early Christian martyrs named Valentine, the most famous being Saint Valentine, executed in the 3rd century CE. One popular legend claims he secretly performed marriages for young couples despite a Roman ban, acts that ultimately led to his execution. While historians debate the accuracy of these stories, they helped cement Valentine’s association with love, sacrifice, and devotion. Love Enters the Story: Medieval Poets Change Everything Valentine’s Day as a romantic holiday didn’t truly take shape until the Middle Ages. English poet Geoffrey Chaucer is often credited with linking February 14 to romantic love in his poetry, helping popularize the idea that it was the day birds chose their mates. From there, the connection between Valentine’s Day and courtly love spread across Europe, especially among the nobility, eventually giving rise to handwritten love notes and tokens of affection. From Handwritten Notes to Hallmark By the 18th and 19th centuries, Valentine’s Day had become a popular occasion for exchanging cards, flowers, and gifts. The Industrial Revolution made printed cards widely available, transforming a once-elite tradition into a mass-market celebration. Today, Valentine’s Day is a global cultural phenomenon, equal parts romance, commerce, and tradition, evolving to include friendships, self-love, and inclusive expressions of connection. It isn’t just about romance, it reflects how traditions evolve over time, absorbing layers of culture, religion, and storytelling. Understanding its history helps explain how societies redefine love, relationships, and celebration across generations. Our experts can help! Connect with more experts here: www.expertfile.com

What Time Should You Actually Turn Off Your Phone at Night?
Everyone’s heard you’re “not supposed to be on your phone before bed” but what does that actually mean in 2026? Most major sleep organizations now recommend putting devices away at least 30–60 minutes before bedtime to protect melatonin and help the brain wind down. The National Sleep Foundation and the American Academy of Sleep Medicine both advise turning off screens about an hour before bed; other experts say a 30–60 minute window is the minimum. (Advisory) Research on blue light shows that evening screen exposure suppresses melatonin and delays sleep, especially when you’re scrolling something stimulating. (Sutter Health) Psychotherapist Harshi Sritharan, MSW, RSW, who specializes in ADHD and digital dependency, puts it bluntly: “To ensure quality sleep and peak performance—whether in sports, work, or school—avoid using your phone after 11 p.m.” For teens and adults with ADHD or anxiety, she says, late-night doomscrolling is especially brutal: screens keep dopamine and stress high at exactly the time the nervous system should be powering down. Harshi says: "The quality of sleep determines your level of executive functioning the next day" She also makes an important distinction: if you are on a device in the evening, active use (choosing a show, talking to friends, looking up something specific) is less harmful than passive use: “Don’t do passive tech use — that doom scrolling, content just being thrown at you,” Sritharan says. “Be more active about your tech use.” That kind of passive feed is more likely to serve up emotionally intense content kids didn’t ask for and aren’t ready to process. You Don’t Need a Perfect Curfew to See Results The good news: the science suggests you don’t have to quit completely at night to feel a difference. A JAMA Network Open study on young adults found that reducing social media use for just one week — not going cold turkey — led to about a 24.8% drop in depression, 16.1% drop in anxiety and 14.5% improvement in insomnia symptoms. Offline.now founder Eli Singer argues that the real challenge is confidence, not willpower. Their data show 8 in 10 people want a healthier relationship with tech, but more than half feel too overwhelmed to know where to start. The platform’s behavior data also show that late afternoons and evenings are when phones dominate use and when people are actually most motivated to make changes. We have less in the tank at night, don't trust willpower to transition off. Have a system/routine of pre-decided of low-effort (potentially fun) activities to help the transition off phones. “We tell people: don’t start with a perfect 8 p.m. curfew,” Singer says. “Start with one realistic phone-off window — even 30 minutes before bed — and prove to yourself you can protect that. That first win matters more than an ideal schedule you’ll never keep.” A Simple, Science-Aligned Answer For most people, Offline.now’s experts land on a practical, high-compliance answer to the question “What time should I turn off my phone?” Aim to put your phone away 30–60 minutes before your target bedtime Make everything after that screen-free by default (books, stretching, music, talking, journaling) If you must be on a device late, keep it brief, low-drama and intentional — no infinite feeds, no emotionally loaded content It’s a small change, but in the context of a day where we’re already on screens for roughly 10 of our 16 waking hours, that last hour matters. Featured Experts Harshi Sritharan, MSW, RSW – Psychotherapist specializing in ADHD, anxiety, insomnia and digital dependency. She explains how late-night and early-morning phone use hijack dopamine, disrupt sleep and make it harder for kids and adults to function the next day. Eli Singer – Founder of Offline.now and author of Offline.now: A Practical Guide to Healthy Digital Balance. He speaks to the platform’s behavioral data on when people are most ready to change, and how 20-minute micro-experiments (like one phone-off window at night) build real confidence over time. Expert interviews can be arranged through the Offline.now media team.




New study suggests Florida Chagas disease transmission
Researchers from the University of Florida Emerging Pathogens Institute and Texas A&M University gathered their resources to investigate the potential of vector-borne transmission of Chagas in Florida. The 10-year-long study, published in the Public Library of Science Neglected Tropical Diseases, used data from Florida-based submissions, as well as field evidence collected from 23 counties across Florida. Chagas disease is considered rare in the United States. Since it is not notifiable to most state health departments, it is quite difficult to know exactly how many cases there are and how frequently it’s transmitted. Chagas disease is caused by the protozoan parasite Trypanosoma cruzi. Nuisance blood-sucking insects known as kissing bugs spread the parasite to humans when exposure to their feces penetrates the mucus membranes, breaches the skin or gets orally ingested. Interestingly, it is believed that most companion animals, like dogs and cats, acquire the parasite from eating the kissing bug itself. The first record of kissing bugs, scientifically known as Triatoma sanguisuga, harboring T. cruzi in Florida was from an insect in Gainesville in 1988. However, kissing bugs have been calling the state home for far longer than humans have. Currently, there are two known endemic species of kissing bugs in the Sunshine State: Triatoma sanguisuga, the species invading homes, and the cryptic species Paratriatoma lecticularia, which live primarily in certain Floridan ecosystems but were not found in this study. Read more ...

We Don’t Realize How Much Time We Spend With AI. Because It’s Hiding in Our Phones
If you ask most people how often they use AI, they’ll say something like: “I tried ChatGPT a couple of times” or “I don’t really use AI.” But look at their phone, and the story is completely different. Digital wellness platform Offline.now has found that we already spend about 10 of our 16 waking hours on screens, roughly 63% of our day. Founder Eli Singer calls AI “the shadow roommate inside those 10 hours”: invisible most of the time, but involved in more of our everyday taps and swipes than we realize. And we now have data to prove it. A recent Talker Research survey of 2,000 U.S. adults, commissioned by Samsung, found that 90% of Americans use AI features on their phones, but only 38% realize it. Common features like weather alerts, call screening, autocorrect, night-mode camera enhancements and auto-brightness are all powered by AI — yet more than half of respondents initially said they don’t use AI at all. Once shown a list of features, 86% admitted they use AI tools daily. (Lifewire) Singer sees this as a classic “confidence gap” problem applied to AI. Beyond the “invisible AI” on our phones, generative AI tools like ChatGPT, Claude and image generators are spreading fast. A nationally representative U.S. survey from Harvard’s Kennedy School and the Real-Time Population Survey found that by August 2024, about 39% of adults aged 18–64 were using generative AI. More than 24% of workers had used it at least once in the previous week, and nearly 1 in 9 used it every single workday. (NBER) Globally, usage is enormous. A World Bank backed analysis of online activity estimated that, as of March 2024, the top 40 generative AI tools attracted nearly 3 billion visits per month from hundreds of millions of users. ChatGPT alone commanded about 82.5% of that traffic. (Open Knowledge Repository) From a mental-health perspective, psychotherapist Harshi Sritharan, MSW, RSW says the issue isn’t just the number of visits, it’s the way AI subtly shapes the texture of our day. “Every autocorrect, every AI-sorted inbox, every ‘magic’ photo fix is a tiny cognitive hand-off,” she explains. “Individually they feel helpful. But taken together, they keep your brain in a constant state of micro-decisions and micro-rewards, which is exhausting, especially if you already struggle with ADHD, anxiety or overwhelm.” She points out that many of her clients only think of “AI time” as the hours they spend in a chatbot window. In reality, AI is involved when: Their phone decides which notifications to surface A map app reroutes them automatically Spam filters silently screen hundreds of emails “By the time they open a dedicated AI app, their nervous system has already been engaging with AI-driven features all day,” Sritharan says. “That’s part of why people end the day feeling tapped out but can’t quite explain why.” Singer worries that this “shadow AI” is quietly eating into the same finite resource Offline.now tracks with screens in general: attention. “We already know 10 hours a day on screens is unsustainable for our focus and our relationships,” he says. “Layer AI on top — systems designed to predict and nudge our behavior — and you’re not just losing time. You’re outsourcing micro-chunks of judgment, memory and choice without even noticing.” So how much time are people spending with AI? Right now, no one has a perfect number and that’s exactly the point. The best data we have suggests: Most smartphone users are already interacting with AI daily, whether they know it or not. (Lifewire) Roughly 4 in 10 U.S. adults now use generative AI, with a growing share using it at work every week or every day. (Harvard Kennedy School) Globally, billions of monthly visits are flowing into AI tools on top of our existing 10-hour screen days. (Open Knowledge Repository) “The future isn’t AI or no AI,” Singer says. “It’s: Can you be conscious about how you use it — instead of letting it hijack your attention and manage your life?” Featured Experts Eli Singer – Founder of Offline.now and author of Offline.now: A Practical Guide to Healthy Digital Balance. He brings proprietary behavioral data on screen time and digital overwhelm, and a framework (the Offline.now Matrix) for rebuilding confidence through 20-minute, real-world steps instead of all-or-nothing “detox” advice. Harshi Sritharan, MSW, RSW – Psychotherapist specializing in ADHD, anxiety and digital dependency. She explains how AI-assisted micro-tasks interact with dopamine, attention and overwhelm, and offers brain-friendly ways to renegotiate your relationship with both screens and AI. Expert interviews can be arranged through the Offline.now media team.