Experts Matter. Find Yours.
Connect for media, speaking, professional opportunities & more.

Baby, It's Cold Outside… And That's No Joke for Seniors
How cold is it? • It's so cold I saw a dog stuck to a fire hydrant. • It's so cold my words froze mid-air and my neighbour had to thaw them out to hear what I said. • It's so cold, I just saw a politician with his hands in his own pockets. Okay, I'm joking—but just a bit. Because while I enjoy a good cold-weather quip, hypothermia isn't funny. Currently, this severe Arctic blast is gripping Canada and large parts of the United States, dropping temperatures 20–40°F (11–22°C) below seasonal norms across a 2,000-mile stretch of North America. Nearly 80 million people are under winter storm warnings. Power outages are anticipated. Roads could be impassable. Travel is about as appealing as a root canal in a snowstorm. For many seniors on both sides of the border, this isn't just an inconvenience—it's a real safety risk. The Cold, Hard Stats (Brace Yourself) Looking at the research I couldn't believe what I found: Older adults are more than 5x as likely to die from hypothermia as younger adults (Kosatsky et al., 2015). In the U.S., approximately half of all hypothermia deaths are people over 65 according to data from the CDC. In Canada, adults over 75 are more than 5 times more likely to die from hypothermia than younger adults—and 87% of those deaths happen right in their own homes. (StatsCan Health Infobase ) Read that again. Slowly. Not on frozen lakes. Not stranded on highways. Instead, in familiar living rooms. Sitting on well-worn couches. Beneath afghans crocheted by someone who loved them. Why Your Body Becomes a Cold -Weather Traitor Our bodies change as we age, and not in the fun "I've earned every wrinkle" way. The insulating fat layer under the skin thins. Circulation slows. Metabolism drops like your interest in small talk. Certain medications—prescription and over-the-counter cold remedies—can interfere with temperature regulation and awareness. Your body's thermostat? It's on the fritz. Here's the math: Hypothermia doesn't require a blizzard. It can begin indoors when temperatures fall below 65°F / 18°C. And here's the truly dangerous part: hypothermia affects the brain first. Judgment declines before shivering becomes severe. You don't realize you're in trouble. You just feel "a bit chilly" while your core temperature quietly drops. Stop Acting Your Age! (But Also... Dress as if you know your age) I'm all for embracing life at every stage—hiking to Everest Base Camp at 60-something, teaching Zumba, and that MBA thing at 70, refusing to "act your age." But embracing life in this weather requires wisdom, not bravado. Cold weather brings real risks: • Slips and falls on icy surfaces (and no, we don't bounce like we used to) • Increased risk of heart attack and stroke because cold thickens the blood • Respiratory infections that linger far too long • Frostbite on fingers and toes • Hypothermia that clouds thinking before any alarms sound. The Indoor Survival Guide—Keep Up (Yes, You Can Get Hypothermia at Home) Set the thermostat to at least 68–70°F (20–21°C). This is not a time to be a miser. Heating bills can be expensive, but hospital stays are even more costly. And they don't even give you warm blankets anymore. Layer like a pro. This is not the time for fashion minimalism. Think: • Long underwear or thermal leggings • Pyjamas under clothes • Stockings or tights under pants • Two pairs of socks • Warm boots with good tread (essential for any outdoor ventures) • Shirts layered under sweaters When it's this cold, if you still own leg warmers—congratulations. Wear them. The warmth is worth the call from the '80s asking for them back. Hats indoors are permitted. This isn't a fashion show; it's survival style. You lose a lot of body heat through your head. Emulate your inner Elmer Fudd if you need to. Carbon monoxide alarms are essential & in many areas legally required. When temperatures drop, people get creative—and desperate. Space heaters, fireplaces, generators, kerosene heaters, or (please, dear God, don't) using gas ovens for heat. That last one is about as safe as texting while skydiving. And here's an important PSA: Starting January 1, 2026, Ontario's updated fire code mandates a functioning carbon monoxide alarm on every level of homes that have fuel-burning appliances. Remember to test alarms when you change your clocks for daylight saving time—it's easy to do, and not easy to forget. Block drafts like you're defending a castle. Roll towels under doors, seal windows, close unused rooms, open curtains during sunny days, and close them tightly at night. Check your medications. Ask your pharmacist or doctor if any prescriptions or over-the-counter remedies influence temperature regulation or alertness. Knowledge is power—and warmth. Check Food & Other Supplies. If venturing out feels risky, order groceries for delivery. Services like Voilà by Sobeys, Instacart, PC Express, and many local grocers deliver directly to your door. This isn't laziness—it's smart risk management. Most delivery services are free or inexpensive, especially when compared to the alternative: icy sidewalks, falls, broken hips, or getting stranded in extreme cold while wearing inadequate footwear because "it's just a quick trip." Clear Your Snow. Snow and ice hinder movement. Limited movement results in isolation. Isolation worsens depression and cognitive decline. Clear snow isn't just about safety—it's about dignity. Pro Tip: Protect Your Pipes (and Your Wallet). Winter power outages can mean burst pipes and serious water damage. If you expect a prolonged outage: • Know where your main water shut-off is • Turn it off • Open faucets to drain the lines It feels extreme—until it doesn't. Until you're standing in three inches of water at 2 a.m., wearing your emergency leg warmers. Know or Live Near an Older Adult? Here's Your Cold Weather Action Plan Don't ask if they need help—just do it. Clear the porch. Shovel a path. Salt the steps. Think of it as the winter cousin of snow angels: shovel angels. Be one! When people Are Shut In—Go check in with them. For those stuck indoors, reach out by video, not just text or voice. Seeing someone tells you far more than hearing "I'm fine." Use FaceTime, Zoom, WhatsApp, or Google Meet. Do this with older people you know. Because pride prevents people from asking for help. Shame prevents people from being honest—about empty fridges, sleeping in mittens, or wearing coats to bed. Look for these signs: • Confusion or slurred speech • Shivering—or lack of it (paradoxically dangerous) • Pale or bluish skin • Slow movements or lack of coordination • Extreme fatigue Know When to Call for Help If something feels off, err on the side of safety. In Canada: • Telehealth Ontario: 1-866-797-0000 • Quebec: 811 • Other provinces: Know your local health line If you notice any signs of distress—confusion, chest pain, shortness of breath, severe cold exposure—or if you're unsure, call 911. Cold-related emergencies escalate rapidly. The Culture Shift We Need—Right Now Cold snaps reveal faults in our systems and communities. This is the time to foster a check-in culture: a call, a knock, a cleared walkway, groceries dropped at the door. Preparation matters. Connection matters more. Winter is temporary. The habits we build to take care of one another are not. Be cool—and stay warm out there, friends. Sue Don’t Retire… Rewire! What are your best winter safety tips? Share them—because staying warm is better when we do it together. Want more of this? Subscribe for weekly doses of retirement reality—no golf-cart clichés, no sunset stock photos, just straight talk about staying Hip, Fit & Financially Free.



Florida scientists champion ‘Food Is Medicine’ movement to tackle national health crisis
University of Florida researchers are calling for a national transformation in how we address the ongoing epidemic of obesity and Type 2 diabetes, starting with a fundamental shift in how we approach health, agriculture and food. Published recently in the Proceedings of the National Academy of Sciences, the article argues that fruits and vegetables must be treated not just as food — but as medicine. With 73% of U.S. adults and 35% of children classified as overweight or obese, the authors warn that the crisis is not only an individual health issue but a national economic and security threat. Andrew Hanson, Ph.D., a co-author and professor of horticultural sciences at UF/IFAS, emphasized a sense of urgency and collective responsibility toward solving this health crisis. “This isn’t business as usual. We’re taking a public-interest view. This is the kind of thing we all need to be talking about. It’s too important not to,” he said. The article proposes a roadmap for change, including creating five National Institutes of Health-supported “Food Is Medicine” centers across the U.S., with Florida as a leading candidate; scaling up domestic fruit and vegetable production to meet national dietary needs; partnering with food producer and processors to make healthy foods more accessible, affordable and appealing; and reforming medical and nutrition education to include horticultural sciences and vice versa. The article highlights that only 1 in 10 adults meets the recommended daily intake of fruits and vegetables, and that U.S. production falls far short of what’s needed to support a healthy population. The authors call for a dramatic expansion of fruit and vegetable production, especially high-impact crops like berries, leafy greens and carrots. Christopher Gunter, Ph.D., professor and chair of the UF/IFAS Department of Horticultural Sciences, said the team’s goal is to push the role fruit and vegetables crops can play in improving human health into the national consciousness. “As a discipline, horticulture and the science of fruit and vegetables have been largely ignored in this conversation,” Gunter said. “Our goal is to move the needle on health with fruit and vegetables.” Hanson said about 80% of the nation’s cropland is used to grow soybeans, corn and wheat — most of which are processed into products with low nutritional value that contribute to the obesity and Type 2 diabetes epidemic. Mike Jaffee, M.D., a co-author and professor of neurology in the UF College of Medicine, stressed the broader implications of a high-vegetable diet on brain health. “Obesity and insulin resistance are linked to inflammation and neurodegeneration. We’re living longer, but our brains aren’t keeping up. That’s where the real cost to individuals and the health care system comes in,” he said. Gunter agreed, adding, “This epidemic reduces the longevity and productivity of our citizens. It limits the momentum communities need to grow healthy and resilient families.” Hanson pointed out that higher socioeconomic groups are better positioned to meet dietary recommendations, making this not just a health issue, but a deeply embedded social and economic one. “This crisis takes an unduly large toll on people with lower incomes and less time. To eat enough fruits and vegetables in the current system, you need substantial income and time to prepare food. That’s a luxury many don’t have,” he said. The authors argue that farmers bring essential knowledge to the table. “They understand how environmental factors impact nutritional quality,” Gunter said.



Anuradha Godavarty, Ph.D., has joined the Virginia Commonwealth University (VCU) College of Engineering, bringing more than two decades of research leadership in optical imaging, medical device innovation and interdisciplinary training to the Department of Biomedical Engineering. “We are thrilled to welcome Dr. Godavarty to our department,” said Rebecca Heise, Ph.D., Inez Caudill, Jr. Distinguished Professor and chair of the Department of Biomedical Engineering. “She is an outstanding scholar and teacher who will expand our collaborations with VCU Health in many applications of optical imaging. Our students and faculty alike will benefit from her experience and mentorship.” Godavarty comes to VCU from Florida International University (FIU), where she served as director of the Optical Imaging Laboratory at FIU. Her work centered on designing and translating near‑infrared optical imaging technologies for clinical use, with applications ranging from breast cancer detection to functional brain mapping to wound assessment. Godavarty has a national reputation for developing portable, low‑cost imaging systems that improve access to care, including hand-held and smartphone-based near‑infrared imaging devices. Her research portfolio includes funding from the National Institutes of Health (NIH), National Science Foundation, Florida Department of Health and American Cancer Society, among others. Godavarty is also a fellow of the American Institute for Medical and Biological Engineering, a senior member of the International Society of Optics and Photonics and the National Academy of Inventors At VCU, Godavarty will expand her research program in optical imaging technologies while collaborating with clinicians, engineers and industry partners across the university and region. Her long‑term goals include advancing bedside imaging tools for wound care, cardiovascular applications and plastic surgery; strengthening global research partnerships; and training the next generation of optical imaging experts. “Virginia Commonwealth University’s engineering and health sciences ecosystem is an ideal place to grow translational research,” Godavarty said. “I look forward to building new collaborations, developing technologies that can make a meaningful difference in patient care and translating these innovations for real-world use by medical professionals.” Godavarty has played a major role in undergraduate education, serving as the undergraduate program director for biomedical engineering at FIU from 2016 to 2022 and leading the department through a successful Accreditation Board for Engineering and Technology (ABET) cycle. She organized FIU’s Annual Diabetes Awareness Day for four consecutive years and regularly engaged K‑12 students through hands-on demonstrations. Throughout her career, Godavarty has been deeply committed to mentoring. In addition to supervising doctoral, master’s and undergraduate students at FIU, she also advised high school students through outreach initiatives and supported several postdoctoral researchers. Her students have earned multiple awards, including NIH and Department of Defense fellowships, national postdoctoral awards and multiple university‑level honors.



The year was 2003, and John Speich, Ph.D., professor in the Department of Mechanical & Nuclear Engineering, felt like he had a clear sense of the direction his burgeoning career was heading in. Speich had recently completed his doctorate in mechanical engineering from Vanderbilt University, where he concentrated on robotics. Following Vanderbilt, Speich went on to become an associate professor at the Virginia Commonwealth University (VCU) College of Engineering, working with students in the Department of Mechanical & Nuclear Engineering. Leveraging his robotics expertise, Speich planned to continue his work developing robotics for medical surgery and rehabilitation. Then Speich got a call from Paul Ratz, Ph.D., a professor at the VCU School of Medicine, asking for assistance that would change the entire focus of Speich’s career. Ratz used a small robotic lever that moved up and down just a few millimeters to stretch tiny strips of bladder muscle and rings of artery, trying to determine how different chemical compounds changed the mechanical properties of the muscle. Speich was intrigued—this was a form of mechanical engineering. “In mechanical engineering, we pull on things to determine the mechanical properties,” says Speich. “Here, Dr. Ratz was pulling on pieces of bladder instead of the typical substances mechanical engineers are known to work with, like steel, aluminum or plastic.” Speich and Ratz began working together in 2003, and now, because of that unique partnership, nearly all of the research Speich does is about the bladder. “Before I started working with Dr. Ratz, I had never even heard the words neurourology or urodynamics,” says Speich. “Now, Neurourology and Urodynamics is the name of the journal I publish in the most.” Today, Speich collaborates on bladder biomechanics with two doctors at VCU Health. Adam Klausner, MD is a urologist and the interim chair of the new Department of Urology at VCU. Linda Burkett, MD is a urogynecologist from the Department of Obstetrics and Gynecology; prior to medical school, Burkett completed her bachelor’s degree in Biomedical Engineering from the VCU College of Engineering. Together, Speich, Klausner and Burkett aim to find non-invasive methods to characterize and diagnose overactive bladder, with the goal of allowing doctors to precisely match patients with the most effective treatments. A number of students across the VCU College of Engineering and VCU School of Medicine have aided in their research, including recent Biomedical Engineering graduate Mariam William. Speich’s primary methods of research involve Near-Infrared Spectroscopy (NIRS)—a non-invasive technology that uses light to measure tissue oxygenation and brain activity—and ultrasound imaging. By using NIRS to study the brain activity associated with the sudden urge to urinate, Speich and his team are working to pinpoint the brain’s role and determine whether it or the bladder is the primary cause of an individual’s condition. “There are a lot of potential causes of overactive bladder,” says Speich. “Some people may have more than one cause. Individual responses to these treatments vary; what works well for one patient may not work at all for the next. We want to give doctors better tools for quantifying information about their patients so they can make better decisions and more optimized treatments.” Thanks to research grants, including a National Institutes of Health (NIH) grant from 2015-2025, Speich has been able to make a number of important findings in his bladder research. His team has closely examined the bladder’s dynamic elasticity, investigating the biomechanical mechanisms that allow the bladder muscle to fill and expand. Another recent focus asks, “Bladder or Brain. Which is it?” Speich and his team developed a tool called a sensation meter that they use to help determine what an individual is feeling as their bladder is filling over time. All this groundbreaking research and medical school collaboration, and to think—Speich nearly missed the opportunity to enter this field entirely. “When I tell students about how I came to be involved in bladder biomechanics, I tell them, you will always keep learning throughout your entire career,” says Speich. “You never know where you’re going to end up. If you’re an engineer, you’re a problem solver, and there are all kinds of problems in areas like business and medicine—beyond the traditional areas people think of when they think of mechanical engineering.”


Sleep Is the First Casualty of Your Screen Habit
Everyone says they want to “sleep better” in the new year. Most start with new pillows, supplements or blackout curtains while the biggest sleep disruptor in the room is still glowing inches from their face. Digital wellness platform Offline.now, founded by author and strategist Eli Singer, has found that we now spend about 10 of our 16 waking hours on screens, roughly 63% of our day. Psychotherapist Harshi Sritharan, MSW, RSW, who specializes in ADHD and modern anxiety, says sleep is often the first system to collapse under that load. Harshi explains that phones and screens emit blue light that hits the retinal ganglion cells in our eyes and tells the brain it’s time to be alert, the opposite of what we need at night: “When we’re leaning towards using our phones right before bed, that blue light hits our system and says, ‘We should be awake.’ It disrupts our circadian rhythm. For people with ADHD or other neurodiversity, whose rhythms are already fragile, adding late-night screen exposure completely throws things off.” She notes that exposure between roughly 11 p.m. and 4 a.m. is particularly damaging for stress and sleep regulation, leaving people “tired all the time throughout the day.” Morning habits can be just as destructive. Sritharan warns that checking your phone first thing essentially programs your brain to chase distraction: “Don’t be on your phone first thing in the morning — it hijacks your attention and your dopamine for the rest of the day. After that kind of stimulation, everything else feels harder and less interesting.” She also calls the snooze button “a pattern that’s making us more tired,” because it fragments REM sleep instead of helping us feel rested. The good news: the data suggests you don’t need a perfect digital detox to see real benefits. A JAMA Network Open study on young adults found that reducing social media use for just one week, not quitting entirely; led to about a 24.8% drop in depression, 16.1% drop in anxiety, and 14.5% improvement in insomnia symptoms. Singer argues that the real barrier isn’t willpower, it’s confidence. Offline.now’s research shows 8 in 10 people want a healthier relationship with tech, but more than half feel too overwhelmed to know where to start. “When people tell us they feel overwhelmed, it’s not laziness. It’s a crisis of confidence,” says Singer. “Lasting change doesn’t require deleting Instagram or TikTok tomorrow. You need to win one personal victory today, and then another tomorrow. That’s how confidence rebuilds.” For journalists covering sleep, mental health, or digital dependency, this story connects the dots between phones, dopamine and insomnia and offers a realistic alternative to the all-or-nothing “digital detox.” Featured Experts Harshi Sritharan, MSW, RSW – Psychotherapist specializing in ADHD, anxiety, insomnia and digital dependency. She explains how blue light, dopamine cycles and “doomscrolling before bed” undermine sleep, especially for neurodivergent clients. Eli Singer – Founder of Offline.now and author of Offline.now: A Practical Guide to Healthy Digital Balance. He speaks to the behavioral data behind digital overwhelm, the confidence gap, and the Offline.now Matrix that turns vague resolutions into actionable micro-steps. Expert interviews can be arranged through the Offline.now media team.




The H³ Plan: How to Retire Without Losing Your Mind & How You Can Support Older Relatives
MEDIA ADVISORY Retirement planning expert Sue Pimento introduces her H³ Plan — a research-backed framework for maintaining mental and emotional health in retirement that goes beyond financial planning. The framework identifies three essential pillars — Hope, Help, and Horizon — that help combat the emotional flatness many retirees experience after leaving structured work. Drawing on neuroscience research and clinical insights, Pimento offers a practical "emotional pension plan" for the growing population of Canadians navigating this life transition. Sue Pimento is available for interviews on retirement wellness, healthy aging, and the psychology of life transitions. Retirement doesn't arrive with a crash. It arrives quietly. One day, you stop setting alarms, stop racing against the clock, stop feeling urgently needed—and no one gives you the mental and emotional playbook for what comes next. There should be a chapter titled: How to Keep Your Brain Engaged, Regulated, and Not Mildly Irritated by Everyone. Instead? 404 page not found. (Translation: the system is actively seeking guidance… and coming up empty.) And if you're nodding along thinking "yes… exactly" — IYKYK. (If You Know, You Know. And if you don't yet, give it time.) Understanding Your Emotional Pension Plan After years of writing, researching, listening, and living through this stage myself, three factors consistently emerge as essential to maintaining mental and emotional health as we age. I call it H³: Hope, Help, and Horizon. Here's why each one matters—and why neglecting any of them leaves you emotionally drained. Think of them as your emotional pension plan — not optional, not fluffy, but essential. 1. Hope: Not Just Wishful Thinking — Agency, Clarified In her reflective New York Times article, "Your Hopes," journalist and believing host Lauren Jackson examines increasing cynicism, waning trust, and—most importantly—what research indicates truly can turn the tide. One line sums up the difference perfectly: Optimism is believing the future will improve. Hope is believing you can make it so. Here's why that matters. Optimism versus Hope (Plain-English Edition) Optimism is passive: "Things will probably work out." Hope is active: "I can influence what happens next." Optimism awaits. Hope takes part. From a psychological perspective, hope is based on: • Agency (I am able to act) • Pathways thinking (I can find a way) Research from the University of Oklahoma's Hope Research Center indicates that hope is one of the strongest predictors of well-being, often surpassing income, education, and even past success. For retirees, this distinction is important because aging narratives often aim to gently remove us from the driver's seat. Hope replies with something more like: Back off, sister. I refuse to buy into outdated stereotypes. I've upgraded to a more modern version of aging—like a new iPod model. (Stereos are out of style. Keep up.) Hope maintains the nervous system in an engaged state rather than resignation. In fact, some see hope as far more nuanced. Frank O’Dea, best known for his personal comeback story — from being homeless to later becoming a very successful coffee entrepreneur as the co-founder of the Second Cup shares his thoughts in his book, “Hope is Not a Strategy.” His personal narrative reinforces a deep belief in hope as a powerful emotional engine, but never as a substitute for action. O’Dea, who later went on to be a co-founder of the Second Cup Coffee Company and is a recipient of the Order of Canada for his philanthropy and humanitarian work, speaks to the human tendency to confuse optimism with preparation — people often wish their way into opportunity, rather than work their way into readiness. I love this line from his book: “Hope is important — it gives us purpose. But without a strategy, it leaves us vulnerable. We win not by wishing, but by working.” — Frank O’Dea 2. Giving Back: Your Brain's Favourite (Unpaid) Job Giving back isn't about virtue. Or virtue signalling on social, for that matter. (It's not a branding exercise. No hashtag required.) It's about nervous system regulation. Over the holidays, I was listening to an interview on CBC Radio and found myself doing that thing where you stop playing Vita Mahjong mid-game because someone said something so logical but also completely fascinating. Gloria Macarenko’s episode with Vancouver-based psychologist and therapist Lawrence Sheppard explored in detail how giving back influences us and what he has personally observed in his practice. The message? Giving back is a key factor for mental health. Certainly, we've all heard the well-known phrase "tis better to give than receive"—or a version of it. But Sheppard wasn't referring to virtue or being kind. He was discussing what truly happens in the brain when we give. Here's the short version: Helping others shifts the brain out of threat mode and into meaning mode. So what's Happening Neurologically? Building on Sheppard's clinical work and broader neuroscience: • Chronic stress forces the nervous system to stay hyper-vigilant. • Rumination shifts inward and intensifies the sense of threat. • Contribution shifts focus outward • Helping activates reward pathways and emotional regulation. Giving back restores balance. • purpose • structure • connection • competence Giving back reminds your brain it's still engaged—just not earning money. (My definition of volunteering. Not Webster's.) And many retirees miss that feeling more than the salary. They also miss the tangibles: vinyl records, 99-cent bread, and the quiet satisfaction of being needed somewhere at 9 a.m. Importantly, giving back—like hope—helps regulate the nervous system by decreasing feelings of isolation and restoring a sense of predictability. Your brain prefers knowing where it belongs. 3. Something to Look Forward To: Anticipation Is Medicine This one is sneaky powerful—and well documented. Having something to anticipate generates excitement. And excitement is not merely a feeling. It's a nervous system event. Here's the connective tissue: All three pillars—hope, giving back, and anticipation—work because they shift the nervous system away from threat and stagnation, and toward engagement, reward, and regulation. The Science (Why Anticipation Works) Research by neuroscientist Wolfram Schultz showed that dopamine spikes most strongly before a reward—not during it. Later studies in affective neuroscience confirmed: • Anticipation boosts motivation and positive emotions. • Future-oriented thinking diminishes depressive rumination. • Predictable positive events enhance mood regulation. In plain English: Your brain lights up when it knows something good is coming. In many instances, anticipation offers more emotional uplift than the event itself. Think: • first date • first kiss • first solo trip • first "I can't believe I'm actually doing this" moment You cannot buy that feeling in a bottle. (Not even the little blue pill will do it.) Why This Matters in Retirement Work used to provide: • deadlines • milestones • future orientation • purpose • feedback • connection • a sense of accomplishment And yes—before anyone writes me a letter—stay-at-home moms, caregivers, and volunteers: that is work. Don't get me started. When structured work concludes, those inputs aren't automatically replaced. Without things to look forward to: • time flattens • mood dulls • life becomes emotionally beige Something—anything—on the calendar restores forward motion. What Giving Back Looks Like in Real Life My friend Janet retired at 63 with a solid financial plan and no emotional plan. Six months in, she was climbing the walls—bored, restless, wondering why she felt so flat when she "should" be enjoying herself. Then she started tutoring at the library (Help), signed up for a pottery course (Horizon), and realized she could actually shape this chapter however she wanted (Hope). Different person. Same retirement account. Completely different nervous system. Big Things Are Overrated Waiting for something big to look forward to is often just perfectionism wearing a sensible cardigan. We tell ourselves the next big milestone will fix everything, when in reality, progress usually happens in a game of inches. Small choices, taken consistently, create big shifts. Direction beats intensity every time. As I wrote in my last blog about my Everest Base Camp and MBA journey: Even Cs get degrees. And I'll add: Consistent B- work wins most races. Small counts: • weekly plans • standing dates • tickets bought months ahead • regular commitments Anticipation is hope with a calendar invite. The H³ Framework for a Happy Retirement (Hope. Help. Horizon.) All three regulate the nervous system and keep us engaged. Hope — I can still shape things Help — I'm useful and connected Horizon — My life has forward motion If life feels flat, add one from each column. That's the prescription. Retirement isn't just about slowing down. It's about re-wiring. In plain English: You are not done yet! Remember, hope keeps you engaged. Giving back keeps you grounded. Looking forward keeps you light. Or, translated: A happy retirement isn't passive. It's practiced. A Note for Those Supporting Older Relatives If you have aging parents, relatives, or friends in your life, be on the lookout for signs of depression, resignation, or apathy. The signs are obvious if you're paying attention: flat affect, repetitive complaints, withdrawal, that vague sense they're just going through the motions, or their smile doesn't reach their eyes. Here's what not to do: point it out directly or suggest they "find a hobby" or "volunteer somewhere." Here's what does work: create Hope and Horizon by scheduling regular outings—lunch, a walk, a movie, anything with a date attached. Sometimes we underestimate how much seniors look forward to our visits and connections. It's better than any tonic or medication to lift spirits, young and old. In this scenario, action speaks louder than words. Talking about depression often brings up shame and further withdrawal. Instead, think of love as a verb, not a noun. You don't need to fix anything. Just show up. Regularly. Predictably. No grand gestures. No reinvention required. Just presence with a pulse - and notifications on mute! Be that person! Don't retire. Re-wire. — Sue Want more of this? Subscribe for weekly doses of retirement reality—no golf-cart clichés, no sunset stock photos, just straight talk about staying Hip, Fit & Financially Free. Subscribe Here
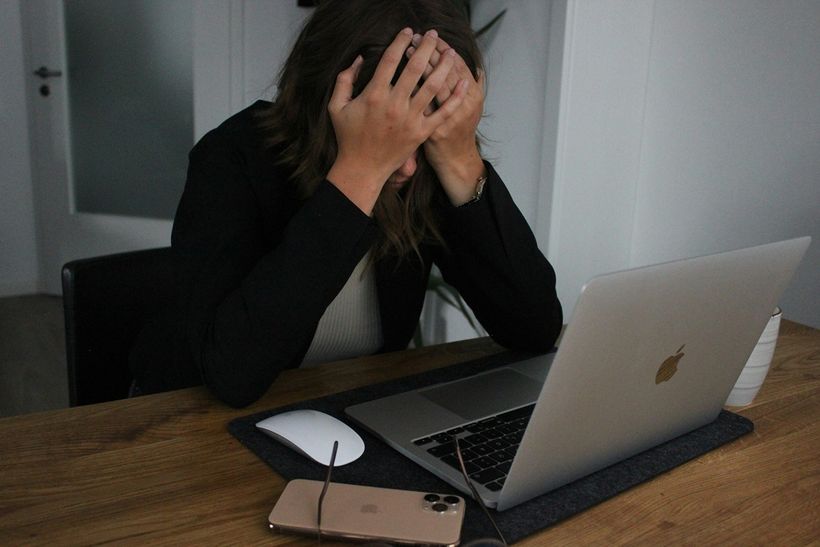
Always On, Never Present: How Work Takes Over Your Life
In many workplaces, being “good at your job” has quietly become synonymous with being constantly reachable. Slack on the laptop, email on the phone, DMs on every platform and a creeping expectation that you’ll answer “just one more thing” at night, on weekends, and even on vacation. Psychotherapist Harshi Sritharan, MSW, RSW and Offline.now founder Eli Singer say this culture is pushing knowledge workers into a state of continuous partial attention: always connected, never fully present. “Most of my high-performing clients don’t have a time-management problem,” says Sritharan. “They have a boundary problem — and their phones are the device enforcing it. Every ping is a tiny dose of dopamine and a tiny spike of stress, and their nervous system never really shuts off.” Research on digital and media multitasking backs up what she sees clinically. Studies have linked frequent task-switching between apps and notifications to: Reduced sustained attention and working memory Slower task performance and more errors Greater mental fatigue and perceived stress Neuroscience and cognition papers also describe how multitasking conditions the brain to seek novelty and micro-rewards, making it harder to tolerate the “boredom” of deep work — exactly the kind of focus most knowledge jobs actually require. Singer argues that the issue isn’t just individual burnout; it’s organizational self-sabotage. Offline.now’s behavioral data show that people now spend about 10 of their 16 waking hours on screens — roughly 63% of the day — and that 8 in 10 want a healthier relationship with tech but feel too overwhelmed to know where to start. “We’ve built workplaces that confuse constant availability with value,” Singer says. “But when you look at the cognitive science, an always-on culture is actually an anti-productivity policy. ‘Do Not Disturb’ isn’t a luxury — it’s the competitive advantage most teams are missing.” The term “continuous partial attention” coined to describe the state of being perpetually attuned to the possibility of new information has been linked in emerging research and commentary to chronic stress, shallow thinking, and emotional exhaustion in modern knowledge work. “The moment you stop treating rest and focus as perks and start treating them as infrastructure, everything changes,” Singer says. “Teams ship better work, people make fewer mistakes, and employees don’t feel like they have to burn their nervous system to keep their job.” For journalists covering work culture, productivity, burnout, or the future of work, this story connects the dots between work apps, multitasking science and mental health and offers a concrete alternative to the “always on” norm. Featured Experts Harshi Sritharan, MSW, RSW – Psychotherapist specializing in ADHD, anxiety, burnout and digital dependency. She helps high-achieving professionals understand how constant notifications, late-night work and screen habits disrupt dopamine, sleep, and emotional regulation — and what sustainable boundaries actually look like. Eli Singer – Founder of Offline.now and author of Offline.now: A Practical Guide to Healthy Digital Balance. He brings proprietary behavioral data on digital overwhelm, the Offline.now Matrix framework, and case examples of organizations reframing “Do Not Disturb” as a strategic asset, not a sign of disengagement. Expert interviews can be arranged through the Offline.now media team.

The health challenges astronauts Butch Wilmore and Suni Williams face after 9 months in space
On June 5, 2024, astronauts Butch Wilmore and Suni Williams embarked on a brief mission to the International Space Station. But equipment failures turned what was supposed to be an eight-day trip into a grueling 9 month spaceflight. This week, Wilmore and Williams finally returned to Earth. While their safe return is cause for celebration, the journey doesn’t end when astronauts touch down on Earth. They now face the significant task of recovering from the physical and psychological toll of long-duration spaceflight. As part of the University of Florida’s ongoing research into astronaut health, Rachael Seidler, Ph.D., a leading expert in spaceflight-associated health changes, is studying the long-term effects of space travel on astronauts’ brains and bodies. Seidler’s research focuses on understanding how the central nervous system and brain structure adapt to the challenges of space travel, as well as how these changes affect performance, balance, and mobility once astronauts return to Earth. “While the physical and psychological challenges astronauts face after returning from long-duration space missions are well-documented, the research we do at UF is helping us understand the intricacies of their recovery process,” said Seidler, deputy director of the Astraeus Space Institute at UF. “By following astronauts like Butch and Suni before, during, and after their missions, we can track how the human body responds to the extreme conditions of space.” Behavioral and Brain Changes Post-Flight Seidler’s research tracks astronauts’ physical and neurological recovery by observing them both during their missions and after they return. "One of the most immediate challenges astronauts face when they return to Earth is mobility and balance. These issues often recover more quickly compared to others, but it takes time for astronauts to readjust to gravity,” Seidler said. "The balance, mobility, and walking difficulties astronauts experience during the first weeks back are typically resolved in a short period, but brain function and structure require longer recovery periods." Seidler’s research indicates that astronauts’ brains exhibit compensation when they return to Earth following spaceflight. This compensation occurs through the recruitment of additional neural pathways in order to return to their preflight performance levels. However, the recovery of brain function is a gradual process. "This brain functional compensation is typically no longer observed within one to six months post-flight," Seidler said. However, not all changes are reversible. "Brain structural changes, particularly related to fluid shifts in space, show little to no recovery even after six months to a year," Seidler said. Two significant structural changes include the brain physically sitting higher in the skull and the expansion of the brain’s ventricles — fluid-filled cavities in the brain — which can increase in volume by 25% or more. These changes are thought to result from the fluid shifts caused by microgravity, and they present long-term health considerations for astronauts. Long-Term Health Effects: Understanding the Impact As Wilmore and Williams embark on their recovery journey, the long-term impact of these changes becomes a critical focus for researchers like Seidler. "The long-term health impacts are crucial to understand because they could affect how astronauts recover and perform in their daily lives post-mission," she said. Seidler’s team at UF is conducting a new study in which they are tracking astronauts for up to five years post-flight to better understand these long-term effects. "We’ve had astronauts in space for up to a year, and we know how to manage their physical health during those missions," Seidler said. "But the effects of space on the brain and body extend beyond the mission, and our work helps inform strategies to manage recovery." Collaborating with NASA and Studying Spaceflight-Associated Neuro-Ocular Syndrome Seidler's work is also part of a broader collaboration with NASA and other scientists to assess astronaut long-term health. The project is particularly focused on Spaceflight-Associated Neuro-Ocular Syndrome, which affects up to 70% of astronauts. This condition involves structural changes to the eye and optic nerve, leading to vision problems that may impact astronauts’ function. "Neuropsychological assessments can help to measure astronauts’ brain health, while studies of the ocular system help identify potential vision issues that may arise during and after long-duration space missions," she said. Simulating Space Conditions on Earth In addition to studying astronauts on Earth and in space, Seidler’s team conducts experiments to simulate the effects of spaceflight on human physiology. The UF lab runs experiments in head-down tilt bed rest studies, which keep participants lying down for weeks to months at a time to simulate the lack of gravity. "This type of study helps us understand how fluid shifts in the body during space travel affect mobility, balance, and brain structure," Seidler explained. "In addition, other publications have reported that astronauts describe that vestibular galvanic stimulation feels similar to what they experience when they first arrive in space and when they return to Earth. We have equipment to induce these effects in the lab." Looking Toward the Future As space missions continue to grow longer and more complex, UF’s research is more important than ever. "We’re studying these issues now to ensure that future astronauts are prepared for the physical and cognitive challenges that await them in deep space," Seidler said.


ExpertSpotlight: Why Hangovers Hurt (and Why Almost Everyone Gets Them Wrong)
The hangover is the ultimate party plot twist: a night of celebration followed by a morning of regret. Headache, nausea, fatigue, brain fog, these aren’t random punishments for having fun. They’re your body’s way of saying it’s been busy processing alcohol, which acts as a diuretic (hello dehydration), irritates the stomach lining, disrupts sleep, and triggers inflammation. Even “just a few drinks” can tip that balance, especially when sleep is short and water is scarce. One of the biggest myths is that hangovers are all about dehydration. Water helps, but it’s only part of the story. Alcohol breaks down into acetaldehyde, a toxic byproduct that contributes to headaches and nausea. It also messes with blood sugar, expands blood vessels, and fragments REM sleep, which is why you can wake up exhausted even after eight hours in bed. Darker drinks often get blamed too; while congeners (chemical byproducts in darker alcohols) can make symptoms worse for some people, quantity and timing usually matter more than color. Then there’s the cure-all folklore: greasy breakfasts, hair of the dog, miracle supplements. Some comfort foods can help stabilize blood sugar, and anti-inflammatory foods may take the edge off, but no remedy truly “cures” a hangover once it’s underway. Time, hydration, light food, and rest remain the most reliable fixes. Prevention, of course, is king: pacing drinks, alternating with water, eating beforehand, and prioritizing sleep do far more than any next-morning hack. Journalists covering health, lifestyle, or New Year’s recovery stories: connect with experts who can explain the real science behind hangovers, what actually works, what’s wishful thinking, and how our bodies respond to alcohol. Whether you’re debunking myths or offering evidence-based tips, expert insight can turn morning-after misery into a smarter story. Find your expert here: www.expertfile.com

My MBA Journey at 69: Because Apparently, Climbing Everest Base Camp Wasn't Enough
If you watched CBS 60-Minutes host, Cecilia Vega set out on a challenging 10-day trek to Everest Base Camp (EBC) in the Himalayas, for last week's episode, you couldn't help but marvel at the gruelling physical demands and the profound experience of being at the foot of Mount Everest. Her journey, which involved intense training, navigating dangerous suspension bridges, and dealing with extreme altitude, also highlighted the massive industry around Everest and the vital, underappreciated role of the Sherpa community. Her journey is an inspiring look at how we can push our own boundaries. Bravo Cecilia! Vega described hiking Everest Base Camp as "the hardest thing I've ever done physically," battling low oxygen (like breathing through a straw) and fatigue, despite months of training. She experienced sub-freezing temperatures, crossed dizzying suspension bridges, and even witnessed close calls with avalanches, with trusty Sherpas conducting nightly tent checks to ensure her safety. Hiking to Everest Base Camp is hard. I know. Because I did it. At 60 Let me explain. I have a tradition of celebrating milestone birthdays with a bang. When I turned 60, I gave myself six physical challenges — one for each decade lived. The grand finale? Climbing to Everest Base Camp. It was epic, exhausting, and left me with both altitude sickness and lifetime bragging rights. But as I approached 69, I craved something different. Not hiking boots this time — just highlighters. Not mountain peaks — mental peaks. I wanted an intellectual challenge that would prove my brain still had some miles left on it. No oxygen tanks required this time. Just caffeine, reliable Wi-Fi, and an iron will. How I Got Here (And Why I'm Questioning My Sanity) I've always wanted an MBA — partly for the knowledge, but let's be honest, mostly for the prestige. There's something irresistible about joining that club of spreadsheet-loving scholars. For years, I've imagined myself casually tossing around terms like "synergy" and "stakeholder engagement" while sipping something expensive in a sleek business lounge. What I didn't imagine was attempting this after a 46-year hiatus from university. Spoiler alert: It's harder than I thought. Like, significantly harder. Enter the MBA: Twenty-four courses. Two years or so, and approximately one hundred "What was I thinking?" moments. I enrolled at the Sprott School of Business at Carleton University, which offers a generous seniors' discount. I briefly debated whether to ask for the student discount or the seniors' discount — then thought, why not request both? I've earned these wrinkles and this tuition bill. Bonus perks: I qualify for the student medical and dental plans. My classmates use them for wisdom tooth extractions. I'm eyeing the denture clause. Term One: The Tech Tsunami Let's talk about the software situation. Brightspace. Turnitin. eProctor. Excel (the betrayer). Word. APA 7th Edition. And about a dozen other platforms that might as well have been written in Klingon. I expected a gentle introduction — maybe some academic foreplay before diving into heavy coursework. Instead, I was shoved into the deep end with weights tied to my ankles. Each assignment came with a forest's worth of readings, PowerPoint slides, and discussion board posts. I was up at 5 a.m., trying to squeeze in extra hours in the day. (Spoiler: you can't.) Despite decades spent managing teams, I was barely scraping 60% on quizzes — the open-book ones. How is that even possible? Accounting became my personal Everest. People kept telling me, "Excel is your friend." That's a lie. Excel is that friend who borrows your car, crashes it, returns it on empty, and then asks if you've bothered reading the manual. Casualties of War: Family, Friends, and Dottie My family was neglected. My friends assumed I'd entered witness protection. Even my little dog Dottie stopped talking to me. She'd give me this look — a devastating combination of pity and disappointment — every time I said, "Sorry, no walk today. Mommy has to study debits and credits." You haven't experienced true shame until you've been judged by a 10-pound dog wearing a sweater. The Breaking Point (And the Breakthrough) I'll admit it — I had serious moments where quitting felt like the only rational option. The workload was relentless. The jargon was endless. The pressure was overwhelming. I contacted teaching assistants, professors, and even the university librarian, desperately searching for a lifeline. They were all kind and patient. But ultimately, I had to figure it out myself. And somewhere between the caffeine highs and APA citation lows, something clicked. Even Cs get Degrees! By midterm, I began to suspect something radical: perhaps the large amount of work was the real test. Not the material itself, but the sheer volume. Maybe this was the school's way of differentiating dedicated students from curious ones, the serious from the casual observers. Was it possible that the secret to MBA success was learning what not to do? After all, the passing grade is a B- (70%). At this point in my life, I'd be happy with a 71% and a full night's sleep. Hence the title, Even Cs get Degrees! Working Smarter, Not Harder Somewhere between week three and mild hysteria, I made a radical decision: stop trying to do everything. I focused on lectures and study notes instead of drowning in supplementary readings. I prioritized assignments strategically. I stopped pretending perfection was achievable — or necessary. The results were immediate: • My grades improved • My panic attacks decreased • Dottie started making eye contact again I also began scheduling regular Zoom calls with professors and TAs — not just for assistance, but to foster genuine relationships (my lifelong superpower). Once I stopped pretending, I had everything under control; everything truly improved. School life has improved. Home life has also improved. I was finally able to brush my hair again. Slowing Down to Soak It In Next term, I'm taking just one course. Because honestly, what's the rush? I'm not chasing a promotion or striving for a corner office. I'm doing this for myself — for the simple joy of learning and the satisfaction of knowing I still can. I want to enjoy the journey, not rush through it gasping. I want to look forward to lectures rather than fear them. I want my sleep score (and my sanity) restored. The goal isn't speed. It's savouring. What I've Learned So Far Here's what these first two courses have taught me: ✓ I can still learn — even when my brain occasionally reboots mid-sentence ✓ I can focus — especially with enough coffee ✓ I'm still gloriously, endlessly curious ✓ I need sleep (The 5 a.m. club can keep their membership) ✓ I need fun (Revolutionary concept, I know) ✓ I love to learn (Turns out, I always have) ✓ I make mistakes — and they're not terminal ✓ I need help — and I must ask for it ✓ APA 7th Edition is real — and I finally understand what it means (Sort of. Mostly. Sometimes.) ✓ Even Cs or, in my case, a B- get a Degree — consistent, sustainable B- work will win most every race Looking Ahead: The Big 7-0 By the time I graduate, I'll be at least 70 years old. And honestly? I can't think of a better birthday gift for myself. When most people talk about slowing down, I'm actually ramping up. While others are downsizing, I'm uploading assignments at 11:58 p.m. When my friends ask why I do this, I smile and say: "Because I still want to know what I'm capable of." To Be Continued... This is just the beginning of my MBA adventure. I've completed two courses out of twenty-four. Twenty-two more to go — one term at a time, one course at a time, one small victory at a time. I'll update this blog periodically with new stories, fresh insights, and probably more tales of Dottie's disappointment. As We Start the New Year Here's a toast to all of us who refuse to act our age. To everyone starting something new — whether it's an MBA, a marathon, or a pottery class. To everyone who believes it's never too late to learn, to laugh, or to start again. Because learning doesn't stop when you retire. Sometimes, it's only just beginning. Stay tuned for Term Two updates, where I'll tackle another course, hopefully retain my sanity, and continue proving that 69 is just a number (and so is 70, 71, 72...). All the best to you in 2026 and beyond! Sue Don’t Retire… ReWire! Want to become an expert on serving the senior demographic? Just message me to be notified about the next opportunity to become a "Certified Equity Advocate" — mastering solution-based advising that transforms how you work with Canada's fastest-growing client segment. Here's the link to sign up.